Advance directives (AD) are an essential part of the Advance Care Plan (ACP), which aims to improve patient care, quality of life, and reduce health costs.[
The benefits of advance directives include reduction of in-hospital mortality rates, higher levels of patient satisfaction, the accomplishment of patient's wills, and reduction of depression and anxiety in end-oflife, for patients and their relatives.[
Every oncologist treating incurable cancer patients in daily practice recognizes the impact of the discontinuation of anticancer treatment and the beginning of the called Best Supportive Care (BSC) modality of treatment. Despite this, there is a lack of data regarding the association of discontinuation of antitumor treatment with advance directives elaboration and implementation. The primary objective of this study is to evaluate if the moment of discontinuation of antitumor treatment could influence the rates of advance directives.
We perform a retrospective study involving cancer patients in palliative treatment at a university hospital in Brazil. Convenience sampling was made by the registry number of their medical records generated by the hospital's electronic system. Eligibility criteria included patients over 18-years-old at the time of disease, an incurable disease (at diagnosis or at progression) and ongoing palliative treatment. Patients with cognitive impairment or documented inability to make decisions were excluded. For data analysis, the patients were divided into two groups, one with and another without advance directives. The cases were followed from the time of diagnosis of the incurable condition until death.
We select the first living will declaration directly manifested by the patients and documented in their medical record as the advance directive to consider in the analysis. This could refer to any will regarding the place of permanence, place of death, and treatment measures as cardiopulmonary resuscitation, mechanical ventilation, chemotherapy, enteral tubes, dialysis, broad-spectrum antibiotics and blood transfusions.[
As a definition of Best Supportive Care (BSC) we consider any palliative treatment, excluding antineoplastic treatments.[
The study was analyzed and approved by the Ethics and Research Committee of our Institution and is registered in the Brazilian National Database for Scientific Research (Plataforma Brazil) with the number CAAE 71559817.6.0000.5327.
Data were collected retrospectively from electronic medical records by direct analysis of documented information. For patients dying outside the hospital and no death registry in the electronic system, an active search was conducted by telephone contact to assess the outcome details. The patients included in this historical cohort were selected from the attendances realized between 2013-2017 and the data were analyzed between October 2017 and June 2018.
Quantitative variables were described by mean and median. The distribution of the qualitative variables was analyzed using percentages. The statistical analysis was performed with SPSS v.18 using the t -test for continuous variables and the chi-square test for categorical variables. The two groups were compared using uni and multivariable logistic regression. The performance status was dichotomized in ECOG 0-3 vs ECOG 4. Places, where the active treatment was discontinued, were also dichotomized in outpatient scenario (mainly doctor's office) and inpatient setting (including the emergency department, wards and ICU). An adjusted Poisson's regression analysis was done for place and performance status at the moment of the discontinuation of anticancer treatment. To determine the sample size we calculated at least 300 patients estimating approximately 25% prevalence of advance directives, providing 80% power to detect a 2.0 hazard ratio for the association between AD and other variables, with a significance level of 5%. We added 10% of possible losses to reach the final sample size. The missing data were managed with pairwise deletion. A p -value below 0.05 was considered statistically significant.
A total of 390 electronic medical records were accessed and 321 subjects confirmed all eligibility criteria and were included in the analysis. The demographic characteristics of the groups with and without advance directives were balanced and summarized in
| Total 321 pts | Without Advance Directives | With Advance Directives | P-value |
|---|---|---|---|
| 248(77,2%) | 73(22,7%) | ||
| Age (median) Gender | 68 | 69 | 0,946 |
| Female | 138(55,6%) | 35(47,9%) | 0,972 |
| Male | 110(44,4%) | 38(52,1%) | |
| Years in school | |||
| < 8 years | 134(54%) | 39(53,4%) | |
| 8 - 11 years | 63(25,4%) | 19(26,0%) | 0,977 |
| > 11 years Marital Status | 51(20,6%) | 15(20,5%) | |
| Married | 152(61,3%) | 38(52,1)% | |
| Single | 76(30,6%) | 28(38,4%) | 0,366 |
| Divorced | 20(8,1%) | 7(9,6%) | |
| Primary Site of the Tumor Upper Gastrointestinal Tract | 55(22,2%) | 15(20,5%) | |
| Lung | 48(19,4%) | 15(20,5%) | |
| Breast | 23(9,3%) | 6(8,2%) | 0,991 |
| Lower Gastrointestinal Tract | 46(18,5%) | 13(17,8%) | |
| Others | 76(30,6%) | 24(32,9%) | |
| Clinical Stage at Diagnosis 1 | 7(2,8%) | 2(2,7%) | |
| 2 | 34(13,7%) | 8(11%) | |
| 3 | 67(27,0%) | 18(24,7%) | 0,993 |
| 4 | 140(56,5%) | 45(61,6%) | |
| PS ECOG at Diagnosis | 38(15,7%) | 12(16,7%) | |
| 1 | 113(46,7%) | 38(52,8%) | |
| 2 | 51(21,1%) | 10(13,9%) | 0,593 |
| 3 | 35(14,5%) | 12(16,7%) | |
| 4 | 5(2,1%) | 0 | |
| Palliative Chemotherapy Yes | 184(74,2%) | 54(74%) | 0,970 |
| No | 64(25,8%) | 19(26,0%) | |
| BSC registry Yes | 191(77,6%) | 64(87,7%) | 0,077 |
| No | 55(22,4%) | 9(12,3%) | |
| PS ECOG at BSC# | |||
| 0 - 3 | 112(58,6%) | 47(74,6%) | 0,137 |
| 4 | 79(41,4%) | 16(25,4%) | |
| Place at BSC# | |||
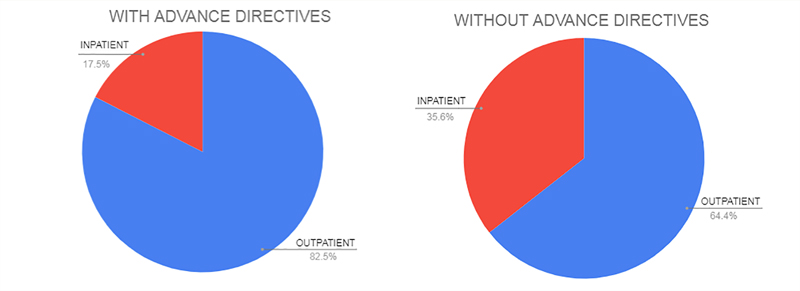
| Outpatient | 123(64,4%) | 52(82,5%) | 0,043 |
| Inpatient+ | 68(35,6%) | 11(17,5%) |
Wald Chi-square test.
Total n=314 pts, due to 7 missing data.
Total n=319 pts, due to 2 missing data (Total patients with BSC registry: 255 due to 11 missing values of AD). # 254 patients due to 1 missing information of PS ECOG and Place at BSC. + Inpatient includes Emergency department, clinical wards, and Intensive Care Unit (ICU). PS ECOG, Eastern Cooperative Oncology Group Scale of Performance Status. BSC, Best Supportive Care.
The group with AD correlated more with the registry of treatment discontinuation compared versus the no AD group (87.7% vs 77.6%) and temporal correlation analysis found that the treatment discontinuation decision occurs on the same day or before the first AD manifestation in 82.3% of cases.
Looking at the moment of treatment discontinuation, the place at this moment seems to correlate in a different way between the groups with and without ADs, as demonstrated in
Figure 1 Places at discontinuation of active treatment and initiation of Best Supportive Care. This graphic illustrates the differences of scenarios between the groups with and without advance directives when Best Supportive Care was initiated.
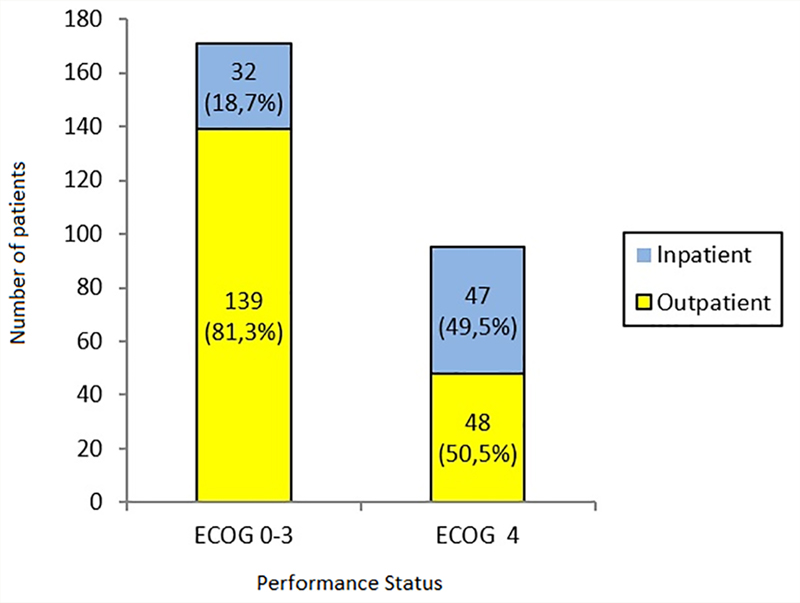
An analysis, independent of the advance directive status, was performed to access the correlation between performance status and place where BSC was implemented. A statistically significant correlation was found between better performance status (PS ECOG 0-3) and the outpatient scenario in comparison with hospitalized patients (RR 1.835; 95% CI 1.387-2.429; p <0.0001), as demonstrated in
Figure 2 Distribution of patients by place and performance status at the moment of BSC decision (n=266). This graphic illustrates the correlation of outpatient scenario with better performance status scores. ECOG: Eastern Cooperative Oncology Group. Inpatient: Emergency, intensive care unit and wards included.
There was no statistical difference in outcomes between the groups with and without an AD. The outcomes included the limitation of therapeutic resources, place of death, receipt of blood components, ICU admissions, invasive palliative procedures (drainage of cavities, biliary tract and derivation of intestinal transit in the majority), the specialty at last assistance, cause of death, orotracheal intubation, mechanical ventilation, artificial parenteral hydration and enteral nutrition, and use of broad-spectrum antibiotics did not differ between groups with and without AD (
| Outcomes | Wthout advance directives | With advance directives | P-value |
|---|---|---|---|
| Place at Limitation of Therapeutic resources (n=267 | 201(100%) | 66(100%) | |
| Clinical Wards | 96(47,8%) | 23(34,8%) | |
| Emergency | 53(26,4%) | 21(31,8%) | 0,230a |
| Doctor's office | 44(21,9%) | 19(28,8%) | |
| ICU | 7(3,5%) | 3(4,5%) | |
| Place of death(n=293 | 232(100%) | 61(100%) | |
| Palliative Unit in the Hospital | 109(47%) | 31(50,8%) | |
| Emergency | 43(18,5%) | 9(14,8%) | |
| Clinical Wards | 38(16,4%) | 11(18%) | 0,905a |
| Home | 25(10,8%) | 5(8,2%) | |
| Other | 10(4,3%) | 2(3,3%) | |
| ICU | 7(3%) | 3(4,9%) | |
| Patients that received Blood transfusions | 136(54,8%) | 41(56,2%) | 0,841a |
| Patients with ICU admission | 14(5,6%) | 5(8,3%) | 0,509a |
| Patients that received Palliative Procedures | 48(20,3%) | 17(25%) | 0,409a |
| Last assistance specialty (n=260 | 204(100%) | 56(100%) | |
| Medical Oncology | 101(48,7%) | 26(46,4%) | |
| Emergency | 42(20,2%) | 9(16,1%) | |
| Palliative Care | 30(14,7%) | 13(23,2%) | 0,738a |
| Internal medicine | 23(11,3%) | 6(10,7%) | |
| Intensive Care | 7(3,4%) | 2(3,6%) | |
| Other | 1(0,5%) | 0 | |
| Cause of Death (n=255 | 200(100%) | 55(100%) | |
| Progression of Disease | 163(81,5%) | 47(85,5%) | |
| Infectious | 28(14%) | 7(12,7%) | 0,396a |
| Vascular | 6(3%) | 1(1,8%) | |
| Other | 3(1,5%) | 0 | |
| Limitation of therapeutic resources Yes | 195(79,6%) | 65(89%) | 0,085a |
| No | 50(20,4%) | 8(11%) | |
| Life-sustaining measures Cardiopulmonary resuscitation | 4/231(1,7%) | 1/61(1,6%) | 0,961a |
| Invasive Airway | 11/231(4,8%) | 3/61(4,9%) | 0,960a |
| Parenteral Hydration | 144/221(65,2%) | 36/59(61%) | 0,555a |
| Artificial Enteral Nutrition | 55/220(25%) | 17/58(29,3%) | 0,505a |
| Broad spectrum antibiotics | 103/222(46,3%) | 30/59(50,8%) | 0,543a |
| Interval between Palliative Diagnosis and Death (median in days) | 464 | 461 | 0,296b |
(A) Pearson chi-square test; (B) Log Rank (Mantel-Cox) Test
Varied values due to missing data in medical records for each outcome ICU, Intensive Care Unit.
The positive correlation between the group with advance directives and the outpatient scenario in the moment of discontinuation of anticancer treatment could be explained by a greater sense of security, confidence and stronger relation with the assistant professional.[
Despite no correlation founded between the performance status and ADs documentation, in daily practice, we observe that the more debilitated patients are less capable to discuss advance care plan and manifest their advance directives. The prognostic impact that poor performance status carries may reinforce mercy feelings by oncologists and/or family members.[
A fact that suggests the presence of collusion in this study population is that despite low rates of ADs, low rates of life-sustaining measures were verified. We also know that patients on PS ECOG 4 also have more cognitive dysfunctions and weaknesses that may compromise their interest and ability to formulate advance directives in time to honor their living wills.[
The 22.7% prevalence of advance directives found in our study is below that described in North America but is consistent with data from other localities.[
Where the oncologic patients have died is an important topic. A large cross-national study involving people with cancer found a large variety of in-home deaths ranging from 12-57%.[
Although the literature indicates a correlation of the advance directives with a reduction in the adoption of aggressive and life-sustaining measures in the terminal setting, in this study the presence of living wills did not statistically correlate with less life-sustaining treatments.[
We must consider that, like any observational study, this research is subject to observational study biases and the results serve as a hypothesis generator. Although it is not able to directly establish a causal relationship, it provides a statistically significant correlation between advance directives registration and the outpatient setting when the anticancer treatment was discontinued, something based on the theoretical rationale. This type of observational data brings the possibility to change practice improving care of palliative cancer patients by discussions and elaboration of advance directives, patients the opportunity to have their wills honored. Finally, we should always keep in mind the multifactorial pattern that influences the composition of advance directives and impaired solid base evidence in this field of research. (
Advanced directives in Brazil, Latin America and all around the world need to be further studied from a clinical perspective, in addition to the legal and psychological view. More prospective large-scale studies are needed to add data to the literature, including intervention studies. The present study is the first to demonstrate that the place of discontinuation of antitumor treatment affects the advance directives rates, and is the first study assessing the reality of advance directives amongst oncologic patients in Brazil.
This conclusion is important if we consider the current development of the therapeutic arsenal and the prolongation of patient survival, with a concomitant gain in quality of life and “chronification” of disease. It brings a natural tendency to postpone the discussion of the advanced care plan to a later moment after all therapeutic lines had failed. The transition to best supportive care could represent a window for discussions about end of life, for the valorization of patient's autonomy, selfdetermination, and to preserve dignity in the death and dying process. In addition, this study suggests that the outpatient scenario is the best for the elaboration of advance directives. Medical assistants should always discuss the aspects of the end of life care with their patient, preferably in the office and on the most appropriate occasions. The focus should always be on dignity and respect for the desires of the patient, from the beginning to the end.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.