Worldwide, oropharynx cancers add up to an estimated 98,412 new cases per year, with an estimated mortality of 48,143 deaths per year.
There is a higher prevalence of squamous cell carcinomas (SCC), which may vary in degrees of invasion and differentiation. Cervical lymph nodes are the most prevalent site of metastasis, with variability from the site of the primary tumor. Local recurrence and local invasion is more common than remote metastasis when treatment failure,
A 50-year-old patient was referred to our service with a history of dysphagia and odynophagia started in June 2020, being submitted to upper digestive endoscopy in an external service with finding of vegetative lesion, without possibility of progression of the apparatus. At physical examination, the lesion was approximately 5cm in the left lateral wall of the oropharynx and adenomegaly (5cm in level II/III to the left and 2cm in level II to the right). Biopsy was performed in our service in August 2020, and a diagnosis of SCC was made. Due to surgical irresectability, referred for final treatment evaluation with chemoradiotherapy.
Before the beginning of the treatment, the patient evolved with respiratory discomfort and cardiorespiratory arrest during endoscopy for passage of the nasoenteral probe, with the need for urgent tracheostomy. Induction chemotherapy was chosen - a scheme with carboplatin + paclitaxel × 3 cycles (from August to October 2020), followed by definitive treatment with concomitant chemotherapy and radiotherapy (cisplatin × 6 weeks), which extended until January 2021.
During treatment the same had fall from his height and trauma in a right upper limb. In March 2021 he had pain on her right hand, and had a tumor in his hand and was soon referred to orthopedics. She presented a fibroelastic consistency tumor, adhered to deep planes, with about 6 cm in diameter in the dorsal region of transition between wrist and right hand, with limited flexion of fingers, as well as limited extension; no sensory deficit (
Figure 1 Fibroelastic consistency tumor, adhered to deep planes, with about 6 cm in diameter in the dorsal region of transition between wrist and right hand, with limited flexion of fingers.
Figure 2 Fibroelastic consistency tumor, adhered to deep planes, with about 6 cm in diameter in the dorsal region of transition between wrist and right hand, with limited flexion of fingers.
Re-staging was requested and biopsy was scheduled after MRI. In imaging tests performed in March and April 2021, the disease progressed in the lung, and extensive expansive lesion affecting soft parts and bone structures at carpus and metacarpal level (
Figure 3 Expansive lesion affecting soft parts and bone structures at carpus and metacarpal level.
Figure 4 Expansive lesion affecting soft parts and bone structures at carpus and metacarpal level.
Figure 5 Expansive lesion affecting soft parts and bone structures at carpus and metacarpal level.
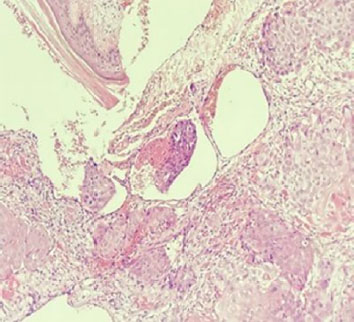
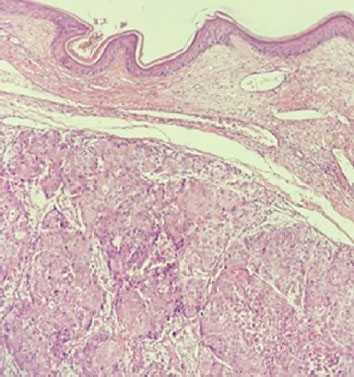
Figure 6 Conventional squamous cell carcinoma, moderately differentiated, involving the deep and reticular dermis, with invasive lymphovascular; overlying epidermis without atypia.
A review conducted by Merino et al. (1977),
Figure 7 Conventional squamous cell carcinoma, moderately differentiated, involving the deep and reticular dermis, with invasive lymphovascular; overlying epidermis without atypia.
The oropharynx consists of the tonsil region (pillars and fossa), base of the tongue, soft palate, and posterior and lateral walls. Carcinoma of these sites is usually squamous and strongly related to smoking and, to a lesser degree, to alcohol intake and some related HPV cases. The most common sites of oropharynx cancer metastasis are cervical lymph nodes, with variability between different levels depending on the position of the primary tumor. An incidence of 70% of lymph node metastasis in oropharynx cancer is estimated, and may be bilateral in up to 50% of cases.
In a study carried out by Liu et al. (2019),
Acrometastasis is rare, studies show an incidence between 0.07% and 0.3%, 50% in the hands and 50% in the feet, the main primary sites found were: lung, breast, and genitourinary. In addition, there is an association of worse prognosis in this patient profile.
Cases of metastasis in soft parts related to head and neck SCC are rare in the literature, with divergent conducts due to the scarcity of cases. They have an impact on quality of life, and may have delayed diagnosis due to unusual presentation. It is critical that one have a pathologist who is dedicated to head and neck. They should be part of the differential diagnosis for patients with pain or edema and the physical examination of the patient in oncologic follow-up should be complete in order to diagnose early.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Goodwin, WJ. Distant metastases from oropharyngeal cancer. J Otorhinolaryngol Relat Spec [online]. 2001, vol. 63, p. 222-3. https://doi.org/10.1159/000055745 Ver referência
2. Globocan 2020, Oropharynx [Internet]. WHO/IARC, 2020.
3. Estimativa 2023: incidência de câncer no Brasil [Internet]. Ministério da Saúde/INCA, 2023.
4. Estimativa 2022: incidência de câncer no Brasil. Ministério da Saúde/INCA, 2022.
5. Kowalski, LP and Carvalho, AL and Martins Priante, AV and Magrin, J. Predictive factors for distant metastasis from oral and oropharyngeal squamous cell carcinoma. Oral Oncol [online]. 2005, vol. 41, p. 534-41. https://doi.org/10.1016/j.oraloncology.2005.01.012 Ver referência
6. Parsons, JT and Mendenhall, WM and Stringer, SP and Amdur, RJ and Hinerman, RW and Villaret, DB. Squamous cell carcinoma of the oropharynx: Surgery, radiation therapy, or both. Cancer [online]. 2002, vol. 94, p. 2967-80.
7. Jesse, RH and Sugarbaker, EV. Squamous cell carcinoma of the oropharynx: why we fail. Am J Surg [online]. 1976, vol. 132, p. 435-8.
8. Troell, RJ and Terris, DJ. Detection of metastases from head and neck cancers. Laryngoscope [online]. 1995, vol. 105, p. 247-50. https://doi.org/10.1288/00005537-199503000-00005 Ver referência
9. Marioni, G and Blandamura, S and Calgaro, N and Ferraro, SM and Stramare, R and Staffieri, A. Distant muscular (gluteus maximus muscle) metastasis from laryngeal squamous cell carcinoma. Acta Otolaryngol [online]. 2005, vol. 125, p. 678-82. https://doi.org/10.1080/00016480410024613 Ver referência
10. Smeets, R and Grosjean, MB and Heiland, M and Riediger, D and Maciejewski, O. Distant metastases of a squamous cell carcinoma of the tongue in peripheral skeletal muscles and adjacent soft tissues. Head Face Med [online]. 2008, vol. 4, p. 7. https://doi.org/10.1186/1746-160X-4-7 Ver referência
11. Merino, OR and Lindberg, RD and Fletcher, GH. An analysis of distant metastasis from squamous cell carcinoma of upper respiratory and digestive tracts. Cancer [online]. 1977, vol. 40, p. 145-51.
12. Marcos, CA and Pendás, JL and Gutiérrez, VF and Hermsen, M and Albalad, MPC and Espina, HF. Distant metastases in head and neck cancer. Acta Otorhininolaringol Esp [online]. 2006, vol. 57, p. 369-72.
13. Samuelian, JM and Fisher, BJ and Daugherty, LC and Babaria, UA. Oropharyngeal squamous cell carcinoma metastatic to lower-extremity soft tissues: a case report and literature review. Ear Nose Throat J [online]. 2013, vol. 92, p. E38-E41.
14. Liu, JC and Bhayani, M and Kuchta, K and Galloway, T and Fundkowski, C. Patterns of distant metastasis in head and neck cancer at presentation: implications for initial evaluation. Oral Oncol [online]. 2019, vol. 88, p. 131-6.
15. Sinha, P and Lewis Junior, JS and Kallogjeri, D and Nussenbaum, B and Haughey, BH. Soft tissue metastasis in p16-positive oropharynx carcinoma: prevalence and association with distant metastasis. Oral Oncol [online]. 2015, vol. 51, p. 778-86.
16. Greco, T and Cianni, L and Mauro, D and Dughiero, G and Bocchi, MB and Cazzato, G. Foot metastasis: current knowledge. Orthop Rev (Pavia) [online]. 2020, vol. 12, p. 8671.





Dados de acesso insuficientes para visualização no mapa.