Merkel cell carcinoma (MCC) is a rare, aggressive, cutaneous malignancy that has a high propensity for recurrence and metastases.
The incidence is higher in men than in women,
MCC incidence increases exponentially with advancing age. In the USA the incidence was 0.1, 1, and 9.8 per 100,000 person-years among individuals aged 40-44, 60-64 and >85 years, respectively.
The Merkel cell polyomavirus can be detected in approximately 80% of all MCCs by real-time polymerase chain reaction (PCR).
In patients with advanced or metastatic MCC, the standard initial treatment options are the checkpoint inhibitors - anti PD-L1 (avelumab)
This case presentation was approved by the ethics in human research committee of the Brazilian National Cancer Institute, Rio de Janeiro, Brazil - CAAE 55545822.6.0000.5274 and all the related procedures were conducted following the good clinical practice guidelines. Written informed consent was provided by the patient.
A 62 years-old female was referred to INCA, in January 2021, reporting a nodular lesion in her left shoulder, with hyperpigmentation and rapid growth since November 2020. The lesion was biopsied and a diagnosis of MCC was made on 01/19/2021, without satellitosis. The immunohistochemistry demonstrated positivity for enolase, chromogranin A and CK20 and negativity for TTF1, LCA and CD68.
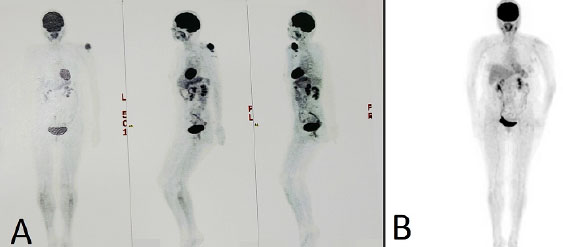
She was submitted to PET-CT on February 5, 2021, showing an expansive lesion with soft tissue density and lobulated borders in the cutaneous/subcutaneous region of the left shoulder, posterior to the humeral head, measuring about 5.0x5.1cm and with a maximum SUV (standard uptake value) of 6.7, associated with other similar nodules adjacent to the described lesion, arranged in subcutaneous tissue of different sizes, including one measuring about 1.8x1.6cm with (SUV 3.1). Prominent lymph nodes in the left axillary region, with a slight increase in the glycolytic metabolism (SUV 1.9) (
Figura 1 A. Initial PET CT in March 2021 demonstrating left shoulder showing an expansive formation with soft tissue density and lobulated borders in the cutaneous/subcutaneous region of the left shoulder, posterior to the humeral head; B. Final PET in August 2021 at the same local, without capitating lesions.
Prior to the prescribed surgical procedure, the result of a SARS-CoV-2 screening swab performed on 03/02/2021 was positive and continued positive on 03/30/2021. She returned for an appointment on 04/01/2021, reporting significant decrease of the lesion, no longer prominent and nodular, being evaluated with residual hyper-pigmented macule. She was submitted to primary tumor resection and sentinel lymph node biopsy on 04/09/2021, with a subsequent histopathological diagnosis of chronic inflammatory process with foreign bodylike gigantocellular reaction and lymphoid follicles in the dermis. No residual neoplasm was identified (
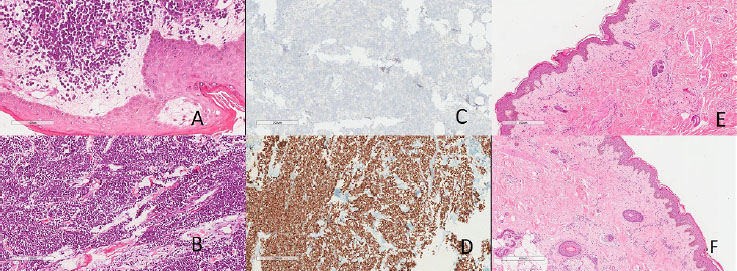
Figura 2 A-B. Initial Biopsy in HE with immunochemistry demonstrating (C) Negative TTF-1 and (D) Positive CK20; E-F. Biopsy of Residual lesion in 04/2021 demonstrating chronicle inflammatory process. At 200x magnification.
On 05/18/2021 the patient was evaluated and only the surgical scar was clinically detected. Due to the possible disease remission, a new PET-CT was performed on 06/08/2021, showing level IIA bilateral cervical lymph nodes (SUV 1.6) with inflammatory aspect.
Discrete radiopaque uptake in the area of densification of subcutaneous cellular tissue in the region posterior to the left humeroscapular joint and axillary joint on the same side (SUV 1.6), probably corresponding to post-surgical alterations, absence of other hyper-metabolic findings suggestive of active neoplastic tissue (
Spontaneous remission after bacterial or viral infection in patients with lymphoma has been reported.
The physiopathology of SARS-CoV-2 (COVID-19) is similar to other respiratory viral diseases, such as influenza, profound lymphopenia may occur in individuals with COVID-19 when SARS-CoV-2 infects and kills T-lymphocyte cells. In addition, the viral inflammatory response, consisting of both the innate and the adaptive immune response, impairs lymphopoiesis and increases lymphocyte apoptotosis.
The authors of this paper did not find any other articles that correlate the interaction between SARS-CoV-2 and MCC.
CONFLICT OF INTEREST
LHRV Manuscript writing
CLCM Manuscript writing
ACM Manuscript writing
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Am Soc Clin Oncol Educ Book [online]. Available from: <>.
2. Ratner, D and Nelson, BR and Brown, MD and Johnson, TM. Merkel cell carcinoma. J Am Acad Dermatol [online]. 1993, vol. 29, p. 143-6.
3. Tilling, T and Moll, I. Which are the cells of origin in Merkel cell carcinoma?. J Skin Cancer [online]. 2012, vol. 2012, p. 680410.
4. Stang, A and Becker, JC and Nghiem, P and Ferlay, J. The association between geographic location and incidence of Merkel cell carcinoma in comparison to melanoma: an international assessment. Eur J Cancer [online]. 2018, vol. 94, p. 47-60.
5. Albores-Saavedra, J and Batich, K and Chable-Montero, F and Sagy, N and Schwartz, AM and Henson, DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol [online]. 2010, vol. 37, p. 20-7.
6. Howard, RA and Dores, GM and Curtis, RE and Anderson, WF and Travis, LB. Merkel cell carcinoma and multiple primary cancers. Cancer Epidemiol Biomarkers Prev [online]. 2006, vol. 15, p. 1545-9.
7. Engels, EA and Frisch, M and Goedert, JJ and Biggar, RJ and Miller, RW. Merkel cell carcinoma and HIV infection. Lancet [online]. 2002, vol. 359, p. 497-8.
8. Paulson, KG and Park, SY and Vandeven, NA and Lachance, K and Thomas, H and Chapuis, AG. Merkel cell carcinoma: current US incidence and projected increases based on changing demographics. J Am Acad Dermatol [online]. 2018, vol. 78, p. 457-63.e2.
9. Melo, AC and Thuler, LCS. Trends in the incidence and morbidity of Merkel cell carcinoma in Brazil. Future Oncol [online]. 2021, vol. 17, p. 2857-65. https://doi.org/10.2217/fon-2020-1313 Ver referência
10. Leroux-Kozal, V and Lévêque, N and Brodard, V and Lesage, C and Dudez, O and Makeieff, M. Merkel cell carcinoma: histopathologic and prognostic features according to the immunohistochemical expression of Merkel cell polyomavirus large T antigen correlated with viral load. Hum Pathol [online]. 2015, vol. 46, p. 443-53.
11. Moghaddam, PA and Cornejo, KM and Hutchinson, L and Tomaszewicz, K and Dresser, K and Deng, A. Complete spontaneous regression of merkel cell carcinoma after biopsy: a case report and review of the literature. Am J Dermatopathol [online]. 2016, vol. 38, p. e154-e8. https://doi.org/10.1097/DAD.0000000000000614 Ver referência
12. Terui, H and Fujimura, T and Kakizaki, A and Furudate, S and Aiba, S. Merkel cell carcinoma with spontaneous regression: a case report and immunohistochemical study. Case Rep Dermatol [online]. 2016, vol. 8, p. 52-8. https://doi.org/10.1159/000444317 Ver referência
13. Kaufman, HL and Russell, J and Hamid, O and Bhatia, S and Terheyden, P and D’Angelo, SP. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol [online]. 2016, vol. 17, p. 1374-85.
14. Kaufman, HL and Russell, JS and Hamid, O and Bhatia, S and Terheyden, P and D’Angelo, SP. Updated efficacy of avelumab in patients with previously treated metastatic Merkel cell carcinoma after ≥1 year of follow-up: JAVELIN Merkel 200, a phase 2 clinical trial. J Immunother Cancer [online]. 2018, vol. 6, p. 7.
15. Nghiem, P and Bhatia, S and Brohl, AS and Hamid, O and Mehnert, JM and Terheyden, P. Two-year efficacy and safety update from JAVELIN Merkel 200 part A: a registrational study of avelumab in metastatic Merkel cell carcinoma progressed on chemotherapy. J Clin Oncol [online]. 2018, vol. 36, p. ASCO#9507.
16. Nghiem, P and Bhatia, S and Lipson, EJ and Sharfman, WH and Kudchadkar, RR and Brohl, AS. Durable tumor regression and overall survival in patients with advanced Merkel cell carcinoma receiving pembrolizumab as first-line therapy. J Clin Oncol [online]. 2019, vol. 37, p. 693-702.
17. Nghiem, PT and Bhatia, S and Lipson, EJ and Kudchadkar, RR and Miller, NJ and Annamalai, L. PD-1 blockade with pembrolizumab in advanced Merkel-cell carcinoma. N Engl J Med [online]. 2016, vol. 374, p. 2542-52.
18. Topalian, SL and Bhatia, S and Hollebecque, A and Awada, A and Boer, JP and Kudchadkar, RR. Non-comparative, open-label, multiple cohort, phase 1/2 study to evaluate nivolumab (NIVO) in patients with virus-associated tumors (CheckMate 358): efficacy and safety in Merkel cell carcinoma (MCC). Cancer Res [online]. 2017, vol. 77, p. CT074.
19. Abe, R and Ogawa, K and Maruyama, Y and Nakamura, N and Abe, M. Spontaneous regression of diffuse large B-cell lymphoma harbouring Epstein-Barr virus: a case report and review of the literature. J Clin Exp Hematop [online]. 2007, vol. 47, p. 23-6.
20. Buckner, TW and Dunphy, C and Fedoriw, YD and Van Deventer, H and Foster, MC and Richards, KL. Complete spontaneous remission of diffuse large B-cell lymphoma of the maxillary sinus after concurrent infections. Clin Lymphoma Myeloma Leuk [online]. 2012, vol. 12, p. 455-8.
21. Yilmaz, F and Yasar, S and Tuncali, MC and Akin, S. Complete response in a frail patient with high-grade B-cell lymphoma to only one cycle of R-CHOP or to prolonged COVID-19?. Semin Oncol [online]. 2021, vol. 48, p. 279-282. https://doi.org/10.1053/j.seminoncol.2021.11.001 Ver referência
22. Zhang, B and Bowerman, NA and Salama, JK and Schmidt, H and Spiotto, MT and Schietinger, A. Induced sensitization of tumor stroma leads to eradication of established cancer by T cells. J Exp Med [online]. 2007, vol. 204, p. e49-e55.
23. Bucktrout, SL and Bluestone, JA and Ramsdell, F. Recent advances in immunotherapies: from infection and autoimmunity, to cancer, and back again. Genome Med [online]. 2018, vol. 10, p. 79.
24. Oliveira, DS and Medeiros, NI and Gomes, JAS. Immune response in COVID-19: what do we currently know?. Microb Pathog [online]. 2020, vol. 148, p. 104484.
25. García, LF. Immune response, inflammation, and the clinical spectrum of COVID-19. Front Immunol [online]. 2020, vol. 11, p. 1441.
26. Wiersinga, WJ and Rhodes, A and Cheng, AC and Peacock, SJ and Prescott, HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19). JAMA [online]. 2020, vol. 324, p. 782-93. https://doi.org/10.1001/jama.2020.12839 Ver referência
27. Li, W and Moore, MJ and Vasilieva, N and Sui, J and Wong, SK and Berne, MA. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature [online]. 2003, vol. 426, p. 450-4.
28. Chen, Y and Guo, Y and Pan, Y and Zhao, ZJ. Structure analysis of the receptor binding of 2019-nCoV. Biochem Biophys Res Commun [online]. 2020, vol. 525, p. 135-40.
29. Letko, M and Marzi, A and Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B beta coronaviruses. Nat Microbiol [online]. 2020, vol. 5, p. 562-9.
30. Xue, X and Mi, Z and Wang, Z and Pang, Z and Liu, H and Zhang, F. High expression of ACE2 on keratinocytes reveals skin as a potential target for SARS-CoV-2. J Invest Dermatol [online]. 2021, vol. 141, p. 206-209.e1. https://doi.org/10.1016/j.jid.2020.05.087 Ver referência
Dados de acesso insuficientes para visualização no mapa.