Uterine carcinosarcoma is a type of malignant neoplasm consisting of mixed histology, with epithelial and mesenchymal components.(
Most women affected by this neoplasm have a mean age of 65 years, and the clinical presentation is similar to that of uterine body tumors, with transvaginal bleeding. In general, they have a low overall survival rate due to late diagnosis and tumor aggressiveness. They often experience locally advanced disease or distant metastases at diagnosis. Metastases occur more frequently by the epithelial component that tends to spread initially lymphatically, as opposed to the sarcomatous component that tends to spread hematogenously. Despite curative treatment, there is a high risk of locoregional and distant recurrences, demanding stricter surveillance.(
Another interesting aspect is that the histology of the tumor apparently revealed that there were two lesions without any connection, something that was later refuted by immunohistochemistry, which revealed, however, that it was the same lesion and that it underwent a transformation called epithelial-mesenchymal transition, a complex phenomenon also described in this article.
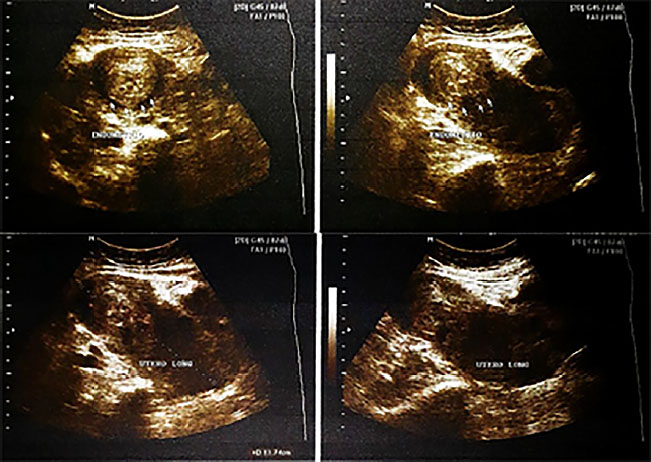
Female patient, white, 59 years old, menarche at 10 years, sexarche at 27 years, menopause at 52 years, G0P0A0, overweight, with hypertension, was admitted to the surgical oncology service with mild pain in the mesogastrium and daily metrorrhagia for six months, interrupted with tranexamic acid. After 2 months of using the medication, she reported pain intensification, from mild to moderate and transvaginal bleeding of small intensity. On physical examination, the uterus was palpable at the level of the umbilical scar and, on the specular examination, a large vegetative lesion was evidenced in the external orifice of the cervical canal and affecting the vaginal wall, friable and foul odor. Pelvic ultrasound detected an endometrial thickening of 25mm, an increased volume of uterus (178cm2) and a heterogeneous echotexture of the cervix (
Figura 1 Pelvic ultrasound showing uterus of regular pear-shaped appearance and surface. Increased volume = 178.6cm3, heterogeneous myometrial echotexture, heterogeneous thickening of the cervix, and the sonographic appearance of the endometrium is irregular (25mm, normal = 5mm). Nonvisualized ovaries. Full bladder, regular surface, shape and normal volumes, in ecostructures inside.
Surgical hysteroscopy showed multiple, voluminous, cystic, friable and tubular vaginal canal lesions. However, there were technical difficulties to overcome the lesion, excising fragments of a polypoid-configuration neoplasm. Histopathological analysis of the fragments showed atypical oval and fusiform cells, some pleomorphic, with round nuclei, evident nucleolus, presence of mitosis, eosinophilic cytoplasm, involving typical endometrial glands, amid loose stroma with areas of recent hemorrhage and necrosis; suggestive of Müllerian adenosarcoma. Pelvis CT reinforced the ultrasound findings. She was then submitted to the surgical procedure, with intraoperative findings of ascitic fluid in moderate amount, topical uterus with the presence of a large mass exceeding the uterine cervix, but without adhesions to the vaginal walls. Total hysterectomy, bilateral adnexectomy and pelvic lymphadenectomy were performed, en bloc resection of the lesion. The patient progressed well, being discharged without complications.
The ascitic fluid revealed a suspicious cytological aspect of neoplastic cells and the pathological study of the material identified two distinct tumors, with no connection between them (
Figura 2 Images of the product of total hysterectomy, weighing 575g, measuring 17.0 x 8.0 x 7.5cm, with smooth serosa and evident vessels. The larger lesion measured 11.5 x 9.5 x 7.5cm, with 0.1cm thickness, the surface is white, externally vegetative and friable. The smaller lesion measured 9.5 x 8.5 x 6.5cm, with a white and friable surface.
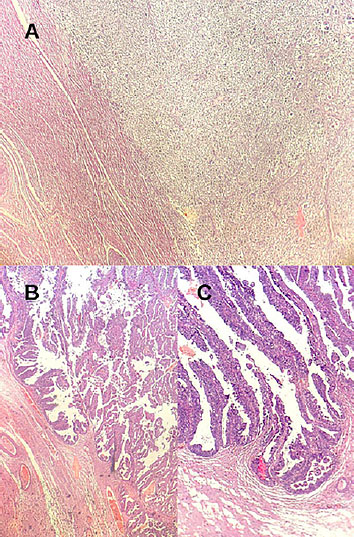
Figura 3 A. Histological sections stained in HE shows endometrial neoplasm with atypical round cell component, with inconspicuous cytoplasmic limits, large nuclei, sparse chromatin, arranged incohesively, with stretches of myxoid stroma. In a smaller increase, neoplastic tissue intersecting with normal myometrium on the right; B. Presence of neoplasia of epithelial origin, forming primitive glands that invade the myometrium, with cells of pleomorphic, hyperchromatic nuclei, conspicuous nucleoli, in addition to mitoses; C. Epithelial tissue invading the myometrium, with cells of distinctly neoplastic characteristics. In greater increase than the anterior image.
| Immunohistochemistry | ||
|---|---|---|
| Antibody | Clone | Result |
| Actin smooth muscle (alpha) | 1 to 4 | Negative |
| Anticytokeratin | 5.2 CAM | Negative |
| CD10 | 56C6 | Positive in rare cells |
| CD99 | 12e7 | Negative |
| CD117 | Polyclonal | Negative |
| Cyclin D1 | SP4 | Negative |
| Cytokeratin | AE1/AE3 | Negative |
| CK7 | OV-TL 12/30 | Negative |
| CK20 | Ks 20.8 | Negative |
| Desmin | D33 | Positive |
| RHEA | E29 | Negative |
| PAX8 | MRQ-50 | Negative |
| RE | SP1 | Negative |
| RP | 1e2 | Negative |
| WT-1 | 6F-H2 | Nuclear negative |
Carcinosarcomas, also called malignant mixed Müllerian tumors, are endometrial carcinomas with a malignant sarcomatous component, which can assume homologous or heterologous elements.(
The incidence of carcinosarcomas is less than 5% of malignant neoplasms of the uterus.(
The reported patientis nulliparousandoverweight, which are considered risk factors because they allude to states of chronic hyperestrogenism. The association of tamoxifen, metabolic syndrome, early menarche, late menopause, and exogenous estrogen exposure isolated with endometrial hyperplasia, proliferative endometrial lesions and endometrial adenocarcinoma is also well established.(
The epithelial-mesenchymal transition is a process in which epithelial cells lose intercellular support and adopt a phenotype similar to that of the mesenchymal, through cytoskeletal remodeling and alteration of migratory activity (increasing the ability to generate metastases).(
Four theories concerning the histogenesis of carcinosarcomas are reported. They are theories of collision, combination, conversion, and composition.(
The monoclonal origin of carcinosarcoma is well established, so that immunohistochemistry shows great agreement between both components. However, some studies still cite the collision of the two biclonal lineages of different progenitor cells as a possible genesis of these tumors. The characterization of mutations and the genetic profile of carcinosarcomas has been improved with sequencing methods. The most common mutations are those of the genes PTEN, PARP1, TP53, PIK3/AKT/MTOR, FBXW7, CCNE1, CHD4, HER2, ARID1A among others; and the TP53 mutation is the most present. Other genetic associations include mutations in KRAS, PPP2R1A and BCOR, as well as abnormalities in the expression of H2A/H2B histones.(
The most prevalent symptom is postmenopausal transvaginal bleeding or premenopausal intermenstrual transvaginal bleeding. Other less common symptoms are palpable mass, pelvic pain, and urinary and fecal changes.(
The diagnosis usually occurs after the pathological study of the entire surgical specimen, since, macroscopically, a carcinosarcoma is indistinguishable from an endometrial carcinoma.(
Among the markers researched in immunohistochemistry from the total hysterectomy, only desmin and CD10 antibodies were positive in rare cells. The other ones were negative and, considering these results and the study of the surgical specimen, the most compatible diagnosis was high-grade papillary serous carcinoma with dedifferentiation to high-grade sarcoma through epithelial-mesenchymal transition (Figure 3). It is worth mentioning that pathologists consider carcinosarcoma as a high-grade endometrial carcinoma, both the pattern of recurrence and metastasis is very similar to that of carcinoma and not to sarcoma.(
Treatment is multimodal, with adjuvant surgery and chemotherapy and/or radiotherapy. Surgery is the main modality of initial treatment and has as objective complete cytoreduction (without macroscopic residual disease) or optimal cytoreduction (residual disease <1cm) and consists of total hysterectomy with bilateral salpingo-oophorectomy, omentectomy, pelvic lymphadenectomy and retroperitoneal, and can be performed openly or minimally invasively (laparoscopic or robotic). According to the guidelines of the European Society for Medical Oncology (ESMO) in the clinical practice guideline, concomitant or sequential chemotherapy and EBRT (external beam radiotherapy) are recommended even in the initial cases.(
The metastases are more derived from the epithelial component, and may, however, present metastasis of the sarcomatous component, or both. The epithelial component is initially disseminated lymphatically, while the mesenchymal component spreads loco-regionally or it is hematogenously disseminated, affecting lung, liver and bone.(
This study is interesting, in this perspective, because, considering these data, the present report would not be in accordance with the speculation that the lesions with metastases due to sarcomas were, in fact, due to the collision of two different tumors, according to the histological report that initially revealed to be distinct lesions with no connection to each other. However, the immunohistochemical study of the piece clarified that it was a monoclonal lesion, which had undergone metaplastic transdifferentiation from carcinoma to sarcoma, contrary to the collision theory presented by those authors.
Previous studies have indicated that the indications of aggressiveness came mainly from the epithelial component, since a serous or clear cell component is more associated with metastases, with greater lymphovascular invasion, greater depth of myometrial invasion and isthmic and cervical involvement, which are markers of worse prognosis of the disease.(
Other prognostic factors to be considered are myometrial involvement >50% of its thickness, presence of heterologous components, incomplete cytoreduction (residual disease >1cm), proportional predominance of the sarcomatous component in the tumor and presence of compromised pelvic and/or retroperitoneal lymph nodes.(
The neoplasm of this report was staged as IIIC1 because it presented pelvic lymph node metastasis by the sarcomatous component, according to the staging of the FIGO. It is noteworthy that, macroscopically, the lesion consisted mainly of sarcoma.
The overall survival rate is very low and prognosis is more reserved than in other gynecological tumors with a similar high degree of carcinogenesis,(
This paper presents a case of uterine carcinosarcoma, a biphasic tumor whose behavior is still little known in a 59-year-old patient with risk factors for the development of uterine cancer.(
YESB Collection and assembly of data, Conception and design, Data analysis and interpretation, Manuscript writing
ACXL Collection and assembly of data, Conception and design, Manuscript writing
CDC Conception and design, Manuscript writing
RPC Manuscript writing
MLVC Conception and design, Final approval of manuscript, Manuscript writing
RMLVL Conception and design, Final approval of manuscript, Manuscript writing
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Zhao, S and Bellone, S and Lopez, S and Thakral, D and Schwab, C and English, DP. Mutational landscape of uterine and ovarian carcinosarcomas implicates histone genes in epithelial-mesenchymal transition. Proc Natl Acad Sci USA [online]. 2016, vol. 113, p. 12238-43. https://doi.org/10.1073/pnas.1614120113 Ver referência
2. Matsuo, K and Ross, MS and Machida, H and Blake, EA and Roman, LD. Trends of uterine carcinosarcoma in the United States. J Gynecol Oncol [online]. 2018, vol. 29, p. e22. https://doi.org/10.3802/jgo.2018.29.e22 Ver referência
3. Lopez-Garcia, MA and Palacios, J. Pathologic and molecular features of uterine carcinosarcomas. Semin Diagn Pathol [Internet] [online]. 2010, vol. 27, p. 274-86.
4. Cherniack, AD and Shen, H and Walter, V and Stewart, C and Murray, BA and Bowlby, R. Integrated molecular characterization of uterine carcinosarcoma. Cancer Cell [Internet] [online]. 2017, vol. 31, p. 411-23.
5. Chen, T and You, Y and Jiang, H and Wang, ZZ. Epithelial-mesenchymal transition (EMT): a biological process in the development, stem cell differentiation, and tumorigenesis. J Cell Physiol [online]. 2017, vol. 232, p. 3261-72. https://doi.org/10.1002/jcp.25797 Ver referência
6. Kord, A and Rabiee, B and Elbaz Younes, I and Xie, KL. Uterine carcinosarcoma: a case report and literature review. Case Rep Obstetr Gynecol [Internet] [online]. 2020, vol. 2020, p. 8816348.
7. McCluggage, WG. Malignant biphasic uterine tumours: carcinosarcomas or metaplastic carcinomas?. J Clin Pathol [online]. 2002, vol. 55, p. 321-5. https://doi.org/10.1136/jcp.55.5.321 Ver referência
8. Borrego, SN and Lengyel, E and Kurnit, KC. Molecular characterizations of gynecologic carcinosarcomas: a focus on the immune microenvironment. Cancers [Internet] [online]. 2022, vol. 14, p. 4465.
9. Zhang, Y and Weinberg, RA. Epithelial-to-mesenchymal transition in cancer: complexity and opportunities. Front Med [Internet] [online]. 2018, vol. 12, p. 361-73.
10. Koskas, M and Amant, F and Mirza, MR and Creutzberg, CL. Cancer of the corpus uteri: 2021 update. Int J Gynecol Obstet [online]. 2021, vol. 155, p. S45-S60. https://doi.org/10.1002/ijgo.13866 Ver referência
11. Brito, PA and Silverberg, SG and Orenstein, JM. Carcinosarcoma (Malignant mixed müllerian (mesodermal) tumor) of the female genital tract: immunohistochemical and ultrastructural analysis of 28 cases. Hum Pathol [Internet] [online]. 1993, vol. 24, p. 132-42.
12. Harano, K and Hirakawa, A and Yunokawa, M and Nakamura, T and Satoh, T and Nishikawa, T. Prognostic factors in patients with uterine carcinosarcoma: a multi-institutional retrospective study from the Japanese Gynecologic Oncology Group. Int J Clin Oncol [Internet] [online]. 2016, vol. 21, p. 168-76.
13. Matsuo, K and Takazawa, Y and Ross, MS and Elishaev, E and Podzielinski, I and Yunokawa, M. Significance of histologic pattern of carcinoma and sarcoma components on survival outcomes of uterine carcinosarcoma. Ann Oncol [Internet] [online]. 2016, vol. 27, p. 1257-66.
14. Menderes, G and Schwab, C and Lopez, S and Black, J and Bellone, S and Silasi, A. Mutational landscape of uterine and ovarian carcinosarcomas. J Clin Oncol [online]. 2016, vol. 34, p. S5589.
15. Ribatti, D and Tamma, R and Annese, T. Epithelialmesenchymal transition in cancer: a historical overview. Transl Oncol [Internet] [online]. 2020, vol. 13, p. 100773.
16. Thompson, L and Chang, B and Barsky, SH. Monoclonal origins of malignant mixed tumors (carcinosarcomas): evidence for a divergent histogenesis. Am J Surg Pathol [Internet] [online]. 1996, vol. 20, p. 277-85.
17. Somarelli, JA and Boss, MK and Epstein, JI and Armstrong, AJ and Garcia-Blaco, MA. Carcinosarcomas: tumors in transition?. Histol Histopathol [online]. 2015, p. 673-87. https://doi.org/10.14670/HH-30.673 Ver referência
18. Ravishankar, P and Smith, DA and Avril, S and Kikano, E and Ramaiya, NH. Uterine carcinosarcoma: a primer for radiologists. Abdom Radiol [Internet] [online]. 2019, vol. 44, p. 2874-85.
19. Cantrell, LA and Blank, SV and Duska, LR. Uterine carcinosarcoma: a review of the literature. Gynecol Oncol [Internet] [online]. 2015, vol. 137, p. 581-8.
20. Chiu, HC and Li, CJ and Yiang, GT and Tsai, APY and Wu, MY. Epithelial to mesenchymal transition and cell biology of molecular regulation in endometrial carcinogenesis. J Clin Med [Internet] [online]. 2019, vol. 8, p. 439.
21. Lu, KH and Broaddus, RR. Endometrial cancer. N Engl J Med [online]. 2020, vol. 383, p. 2053-64. https://doi.org/10.1056/NEJMra1514010 Ver referência
22. Ribeiro, B and Silva, R and Dias, R and Patrício, V. Carcinosarcoma of the uterine cervix: a rare pathological finding originating from mesonephric remnants. BMJ Case Rep [online]. 2019, vol. 12, p. e227050. https://doi.org/10.1136/bcr-2018-227050 Ver referência
23. Emoto, M and Iwasaki, H and Ishiguro, M and Kikuchi, M and Horiuchi, S and Saito, T. Angiogenesis in carcinosarcomas of the uterus: differences in the microvessel density and expression of vascular endothelial growth factor between the epithelial and mesenchymal elements. Hum Pathol [online]. 1999, vol. 30, p. 1232-41.
24. Freeman, SJ and Aly, AM and Kataoka, MY and Addley, HC and Reinhold, C and Room, E. The revised fig staging system for uterine malignancies: implications for MR imaging. RadioGraphics [online]. 2012, vol. 32, p. 1805-27. https://doi.org/10.1148/rg.326125519 Ver referência
25. D’Angelo, E and Prat, J. Uterine sarcomas: a review. Gynecol Oncol [Internet] [online]. 2010, vol. 116, p. 131-9.
26. Oaknin, A and Bosse, TJ and Creutzberg, CL and Giornelli, G and Harter, P and Joly, F. Endometrial cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol [Internet] [online]. 2022, vol. 33, p. 860-77.
27. Sreenan, JJ and Hart, WR. Carcinosarcomas of the female genital tract. A pathologic study of 29 metastatic tumors: further evidence for the dominant role of the epithelial component and the conversion theory of histogenesis. Am J Surg Pathol [online]. 1995, vol. 19, p. 666-74.

Dados de acesso insuficientes para visualização no mapa.