Poly(ADP-ribose) polymerase (PARP) inhibitors represent a major step forward in the treatment of various types of solid tumors characterized by specific defects in DNA repair mechanisms, such as deleterious BRCA1 and BRCA2 mutations and other types of homologous-recombination deficiency (HRD).
Following the positive results observed in the platinum-sensitive recurrent disease, recent phase 3 trials have investigated different PARP inhibitors in the front-line setting as maintenance for patients with advanced EOC and germline or somatic BRCA1 or BRCA2 mutations, with the evaluation of homologous recombination deficiency (HRD), using the myChoice® test (Myriad Genetics).
The expert panel was composed of 20 medical oncologists from Brazil with a professional focus on gynecological oncology, especially ovarian cancer. The panel was organized by a committee composed of four of the current authors (AC, DXA, FCM, and GZDM), who created the multiple-choice questions addressed by the panel and coordinated its conduct. The questions aimed to elicit recommendations on salient issues that pertain to the use of PARP inhibitors only in the front-line management of patients with high-grade EOC. The use of PARP inhibitors in other scenarios, as maintenance after platinum sensitive or for patients with platinum-resistant disease were not included in this consensus. The two PARP inhibitors approved in Brazil as of March 2021 (niraparib
Results for each of the 67 questions addressed by the panel were analyzed descriptively and grouped – according to clinical setting or issue – in a manner that eventually allowed for 35 recommendations related to those settings or issues. The 67 questions are provided in the supplementary materials. As a general rule, those questions covered the following sets of issues: (1) which patients should be tested, and when; (2) what test should be used; (3) when should maintenance PARP inhibitor therapy be indicated; (4) what agent should be used; (5) when should bevacizumab be combined; and (6) what toxicity should be expected and how should it be managed. For each question, if at least 75% of the voting panel members selected a particular answer, a consensus was considered to be present. If between 50.0% and 74.9% of the voting members selected a particular answer, this was considered as majority vote, but no consensus. When not even majority vote was present, the recommendation was still provided, in this case under the rubric of “no consensus”, which indicates that even if there was a predominant answer, it did not reach 50.0% of the votes. For each question, a response option “abstain” was to be chosen when a member felt impeded to provide a qualified response for any reason.
The panel was made possible by educational grants from GlaxoSmithKline and AstraZeneca. These financial sponsors did not influence the creation of the questions, the panel conduct, or the writing of the article, all of which rested under the entire responsibility of the authors.
There is no consensus on which histology should be tested for BRCA mutations.
There is consensus that testing should take place upon diagnosis, regardless of stage.
There is consensus that testing can be performed on saliva, blood, or tumor.
By majority vote, testing should first be performed on saliva and/or blood. If these are negative, there is consensus to do somatic test.
By majority vote, a next-sequencing generation (NGS) panel with more than 12 genes should be used to assess germline alterations in BRCA1 , BRCA2, and other genes involved in homologous recombination pathways and mismatch repair complex.
By majority vote, testing must be broad when a somatic panel is used. By consensus, myChoice® (Myriad Genetics) is considered standard for HRD evaluation.
There is no consensus on reasons for not performing BRCA testing, even though lack of access and cost are the limiting factors.
By consensus, PARP inhibitors should not be used as maintenance therapy in patients with newly diagnosed, early-stage (I or II) EOC due to lack of data in the literature to support this indication.
By consensus, PARP inhibitors should be used as maintenance therapy in patients with newly diagnosed, advanced-stage (III or IV) EOC.
By majority vote, the presence of BRCA mutation or HRD is a sufficient indication of PARP inhibitors as maintenance therapy for patients with advanced EOC after first-line chemotherapy.
By majority vote, the choice of PARP inhibitor involves access, tolerability, effectiveness, and personal experience.
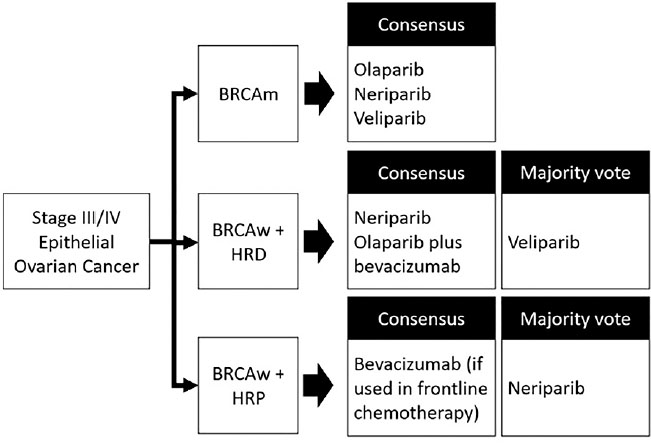
By majority vote, any of the following PARP inhibitors can be recommended for BRCA-mutated patients with advanced EOC after first-line chemotherapy: niraparib, olaparib, or veliparib.
By consensus, niraparib monotherapy is recommended in BRCA-mutated patients and those with HRD. By majority vote, it is also recommended in BRCA wild-type and homologous-recombination proficient patients.
By consensus, olaparib monotherapy is recommended for BRCA-mutated patients and should not be indicated in BRCA wild-type and homologous-recombination proficient patients. However, for patients with HRD, there is no consensus (since 50.0% of the voters were for and 50.0% were against such recommendation).
By consensus, olaparib combined with bevacizumab is recommended for patients with HRD and should not be indicated in BRCA wild-type and homologous-recombination proficient patients.
By consensus, veliparib monotherapy is recommended for BRCA-mutated patients and should not be indicated in BRCA wild-type and homologous-recombination proficient patients. By majority vote, it is also recommended for patients with HRD.
There is no consensus on which PARP inhibitor monotherapy or if Olaparib combined with bevacizumab should be the treatment of choice in BRCA wild-type patients with HRD.
By majority vote, any PARP inhibitor or olaparib combined with bevacizumab may be recommended for BRCA-mutated patients.
By majority vote, niraparib is the recommended PARP inhibitor for BRCA wild-type and homologous-recombination proficient patients.
There is consensus that niraparib can be recommended for BRCA wild-type patients with no HRD testing, in advanced-stage EOC with residual disease.
There is no consensus on whether the duration of PARP inhibitor therapy should follow agent-specific prespecified duration or the presence of residual disease or complete response.
There is no consensus on the first-line chemotherapy regimen of choicein advanced EOC, when considering the options of carboplatin plus paclitaxel; carboplatin plus paclitaxel plus bevacizumab; and carboplatin plus liposomal doxorubicin.
By consensus, bevacizumab is added to carboplatin plus paclitaxel in patients with advanced-stage, BRCA wild-type and HRD tumors undergoing suboptimal cytoreduction.
There is consensus that bevacizumab can be added to chemotherapy only in stage III/IV patients with residual tumor after primary debulking surgery, but no consensus in patients without residual disease.
By majority vote, for BRCA-mutated patients who underwent chemotherapy plus bevacizumab, bevacizumab should be stopped and a PARP inhibitor started. Also, by majority vote, olaparib should be added to bevacizumab for BRCA wild-type and HRD patients. By consensus, bevacizumab monotherapy should be continued for BRCA wild-type and homologous-recombination proficient patients.
There is consensus that the toxicity profiles of PARP inhibitors are different and influence the choice of treatment, but there is no consensus on which one is the best tolerated.
There is no consensus on a PARP inhibitor of choice in patients with hypertension. By majority vote, niraparib should be avoided in patients with severe cardiovascular disease.
By majority vote, there is no support for the choice of a specific PARP inhibitor for patients using multiple medications.
By majority vote, nausea and vomiting should only be treated if the patient develops symptoms, not in a preventive manner. By majority vote, all PARP inhibitors raise the same moderate degree of concern about emesis.
There is consensus that the risk for developing myelodysplastic syndrome or acute myeloid leukemia is low, but all patients should be carefully monitored for hematologic toxicity.
By majority vote, olaparib and veliparib are of moderate concern, while niraparib is of high concern, regarding the incidence of myelosuppression.
By majority vote, weekly blood counts in the first month should be ordered in patients starting niraparib, followed by monthly counts for the first year and periodically thereafter; patients on olaparib and veliparib should be monitored monthly from the start of treatment for 1 year and periodically thereafter.
By consensus, niraparib and veliparib raise low concern regarding the incidence of pneumonitis; by majority vote, olaparib also raises low concern about such a risk. By consensus, the performance of computed tomography of the chest should be guided by symptoms.
By consensus, niraparib and veliparib raise moderate concern regarding the incidence of fatigue. There is no consensus on olaparib.
PARP inhibitors are the first class of agents that allow for precision medicine in the treatment of ovarian cancer. The hallmark of precision medicine is the use of targeted agents based on predictive biomarkers and testing for the presence of such biomarkers plays a central role toward that goal. Several medical societies have provided up-to-date recommendations on counseling and testing for BRCA mutations and HRD in clinical practice, whether more generally or for patients with ovarian cancer in particular.
In keeping with the available results from phase 3 trials, the panel recommends that maintenance therapy with PARP inhibitors should be considered only for patients with newly diagnosed advanced EOC, and not in early-stage disease.
One of the key difficulties faced by practicing oncologists is the choice among different effective agents that have not been subject to head-to-head comparisons, which is currently the case with PARP inhibitors. Therefore, elicitation of majority preference or consensus plays an important role in these cases.
Figura 1 Panel recommendations for three groups of patients defined by BRCA status (m = Mutated; w = Wild-type) or homologous-recombination status (HRD = Homologous-recombination deficient; HRP = Homologous-recombination proficient).
The panel reached no consensus on the firstline chemotherapy regimen of choice in advanced EOC, when considering the standard options.
The frequency and management of toxicity from PARP inhibitors in EOC have been addressed by international practice guidelines and reviews.
The risk of acute myeloid leukemia and myelodysplastic syndrome from PARP inhibitors has been extensively debated in the recent literature, and of particular concern has been the attempt to investigate a potential causal role for both PARP inhibitors and platinum-based therapy.
By providing the current recommendations, the panel wishes to help practitioners from Brazil to improve the care they provide to women with EOC, specifically through the efficient use of PARP inhibitors in the front-line management of newly-diagnosed, advanced disease amenable to derive benefit from this practice-changing class of agents.
AFCC Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
DXA Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
GDM Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
ACM Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
ANR Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
KK Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
APGG Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
MSA Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
CRA Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
DF Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
AMM Collectionandassembly of data, Final approval of manuscript, Manuscript writing
ACL Collectionandassembly of data, Final approval of manuscript, Manuscript writing MC Collectionandassembly of data, Final approval of manuscript, Manuscript writing
JSN Collectionandassembly of data, Final approval of manuscript, Manuscript writing
PS Collectionandassembly of data, Final approval of manuscript, Manuscript writing
EC Collectionandassembly of data, Final approval of manuscript, Manuscript writing
RC Collectionandassembly of data, Final approval of manuscript, Manuscript writing
RG Collectionandassembly of data, Final approval of manuscript, Manuscript writing
EP Collectionandassembly of data, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
FCM Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Ashworth, A. A synthetic lethal therapeutic approach: poly(ADP) ribose polymerase inhibitors for the treatment of cancers deficient in DNA double-strand break repair. J Clin Oncol [online]. 2008, vol. 26, p. 3785-90.
2. Mateo, J and Lord, CJ and Serra, V and Tutt, A and Balmaña, J and Castroviejo-Bermejo, M. A decade of clinical development of PARP inhibitors in perspective. Ann Oncol [online]. 2019, vol. 30, p. 1437-47.
3. Lheureux, S and Gourley, C and Vergote, I and Oza, AM. Epithelial ovarian cancer. Lancet [online]. 2019, vol. 393, p. 1240-53.
4. Kim, J and Park, EY and Kim, O and Schilder, JM and Coffey, DM and Cho, CH. Cell origins of high-grade serous ovarian cancer. Cancers (Basel) [online]. 2018, vol. 10, p. 433.
5. Peres, LC and Cushing-Haugen, KL and Köbel, M and Harris, HR and Berchuck, A and Rossing, MA. Invasive epithelial ovarian cancer survival by histotype and disease stage. J Natl Cancer Inst [online]. 2019, vol. 111, p. 60-8.
6. Morgan, RD and Burghel, GJ and Flaum, N and Bulman, M and Clamp, AR and Hasan, J. Prevalence of germline pathogenic BRCA1/2 variants in sequential epithelial ovarian cancer cases. J Med Genet [online]. 2019, vol. 56, p. 301-7.
7. Pennington, KP and Walsh, T and Harrell, MI and Lee, MK and Pennil, CC and Rendi, MH. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin Cancer Res [online]. 2014, vol. 20, p. 764-75.
8. Bonadio, RRCC and Fogace, RN and Miranda, VC and Diz, M. Homologous recombination deficiency in ovarian cancer: a review of its epidemiology and management. Clinics (Sao Paulo) [online]. 2018, vol. 73, p. e450s.
9. Moore, K and Colombo, N and Scambia, G and Kim, BG and Oaknin, A and Friendlander, M. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med [online]. 2018, vol. 379, p. 2495-505.
10. Coleman, RL and Fleming, GF and Brady, MF and Swisher, EM and Steffensen, KD and Friendlander, M. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med [online]. 2019, vol. 381, p. 2403-15.
11. Gonzalez-Martin, A and Pothuri, B and Vergote, I and Christensen, RD and Graybill, W and Mirza, MR. Niraparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med [online]. 2019, vol. 381, p. 2391-402.
12. Ray-Coquard, I and Pautier, P and Pignata, S and Pérol, D and González-Martín, A and Berger, R. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. [online]. 2019, vol. 381, p. 2416-28.
13. Daly, MB and Pal, T and Berry, MP and Buys, SS and Dickson, P and Domcheck, SM. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw [online]. 2021, vol. 19, p. 77-102.
14. US Preventive Services Task Force. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US preventive services task force recommendation statement. [online]. 2019, vol. 322, p. 652-65.
15. Konstantinopoulos, PA and Norquist, B and Lacchetti, C and Armstrong, D and Grisham, RN and Goodfellow, PJ. Germline and somatic tumor testing in epithelial ovarian cancer: ASCO Guideline. J Clin Oncol [online]. 2020, vol. 38, p. 1222-45.
16. Pujol, P and Barberis, M and Beer, P and Friedman, E and Piulats, JM and Capoluongo, ED. Clinical practice guidelines for BRCA1 and BRCA2 genetic testing. Eur J Cancer [online]. 2021, vol. 146, p. 30-47.
17. Miller, RE and Leary, A and Scott, CL and Serra, V and Lord, CJ and Bowtell, D. ESMO recommendations on predictive biomarker testing for homologous recombination deficiency and PARP inhibitor benefit in ovarian cancer. Ann Oncol [online]. 2020, vol. 31, p. 1606-22.
18. ESMO Guidelines Committee. Updated treatment recommendations for newly diagnosed epithelial ovarian carcinoma from the ESMO Clinical Practice Guidelines. Ann Oncol [online]. 2021, vol. 32, p. 1300-3.
19. Desmond, A and Kurian, AW and Gabree, M and Mills, MA and Anderson, MJ and Kobayashi, Y. Clinical actionability of multigene panel testing for hereditary breast and ovarian cancer risk assessment. JAMA Oncol [online]. 2015, vol. 1, p. 943-51.
20. LaDuca, H and Stuenkel, AJ and Dolinsky, JS and Keiles, S and Tandy, S and Pesaran, T. Utilization of multigene panels in hereditary cancer predisposition testing: analysis of more than 2,000 patients. Genet Med [online]. 2014, vol. 16, p. 830-7.
21. Cham, S and Wright, AA. Underutilization of germline BRCA testing in commercially-insured women diagnosed with ovarian cancer. J Clin Oncol [online]. 2021, vol. 39, p. 5539.
22. Achatz, MI and Caleffi, M and Guindalini, R and Marques, RM and Nogueira-Rodrigues, A and Ashton-Prolla, P. Recommendations for advancing the diagnosis and management of hereditary breast and ovarian cancer in Brazil. JCO Glob Oncol [online]. 2020, vol. 6, p. 439-52.
23. Alemar, B and Gregorio, C and Herzog, J and Bittar, CM and Oliveira Netto, CB and Artigalas, O. BRCA1 and BRCA2 mutational profile and prevalence in hereditary breast and ovarian cancer (HBOC) probands from Southern Brazil: are international testing criteria appropriate for this specific population?. PLoS One [online]. 2017, vol. 12, p. e0187630.
24. Maistro, S and Teixeira, N and Encinas, G and Katayama, MLH and Niewiadonski, VDT and Cabral, LG. Germline mutations in BRCA1 and BRCA2 in epithelial ovarian cancer patients in Brazil. BMC Cancer [online]. 2016, vol. 16, p. 934.
25. Tew, WP and Lacchetti, C and Ellis, A and Maxian, K and Banerjee, S and Bookman, M. PARP inhibitors in the management of ovarian cancer: ASCO Guideline. J Clin Oncol [online]. 2020, vol. 38, p. 3468-93.
26. Banerjee, S and Gonzalez-Martin, A and Harter, P and Lorusso, D and Moore, KN and Oaknin, A. First-line PARP inhibitors in ovarian cancer: summary of an ESMO Open - cancer horizons round-table discussion. ESMO Open [online]. 2020, vol. 5, p. e001110.
27. Oza, AM and Cook, AD and Pfisterer, J and Embleton, A and Ledermann, JA and Pujade-Lauraine, E. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol [online]. 2015, vol. 16, p. 928-36.
28. Tewari, KS and Burger, RA and Enserro, D and Norquist, BM and Swisher, EM and Brady, MF. Final overall survival of a randomized trial of bevacizumab for primary treatment of ovarian cancer. J Clin Oncol [online]. 2019, vol. 37, p. 2317-28.
29. Ledermann, JA. First-line treatment of ovarian cancer: questions and controversies to address. Ther Adv Med Oncol [online]. 2018, vol. 10, p. 1758835918768232.
30. LaFargue, CJ and Dal Molin, GZ and Sood, AK and Coleman, RL. Exploring and comparing adverse events between PARP inhibitors. Lancet Oncol [online]. 2019, vol. 20, p. e15-e28.
31. Xu, Y and Ding, L and Tian, Y and Bi, M and Han, N and Wang, L. Comparative efficacy and safety of PARP inhibitors as maintenance therapy in platinum sensitive recurrent ovarian cancer: a network meta-analysis. Front Oncol [online]. 2020, vol. 10, p. 573801.
32. Madariaga, A and Bowering, V and Ahrari, S and Oza, AM and Lheureux, S. Manage wisely: poly (ADP-ribose) polymerase inhibitor (PARPi) treatment and adverse events. Int J Gynecol Cancer [online]. 2020, vol. 30, p. 903-15.
33. Morice, PM and Leary, A and Dolladille, C and Chrétien, B and Poulain, L and González-Martín, A. Myelodysplastic syndrome and acute myeloid leukaemia in patients treated with PARP inhibitors: a safety meta-analysis of randomised controlled trials and a retrospective study of the WHO pharmacovigilance database. Lancet Haematol [online]. 2021, vol. 8, p. e122-e34.
Dados de acesso insuficientes para visualização no mapa.