Cervical cancer is considered a public health problem. It is the fourth most common cause of cancer among women worldwide and projected to increase from 570,000 to 700,000 cases between 2018 and 2030. The annual mortality rate is projected to increase from 311,000 to 400,000.
The International Federation of Gynecology and Obstetrics (FIGO) classification is used for disease staging. Stage III-B corresponds to invasion into the pelvic wall, hydronephrosis, or a non-functioning kidney.
Currently, the proposed therapy for locally advanced cervical cancer patients is radiation therapy (RT), concomitant with cisplatin-based chemotherapy (CT). Cisplatin is a chemotherapeutic agent that can potentially cause acute tubular necrosis and result in renal failure and is often not prescribed to patients with preexisting renal dysfunction (i.e., GFR<50-60ml//min/1.73m2).
In locally advanced stages IIIB, IIIC2, and IVA, clinical studies have demonstrated that unilateral and bilateral hydronephrosis are predictors of mortality and poor prognostic factors for survival. Urinary diversion procedures using percutaneous nephrostomy (PCN) or ureteral stents are available options for such cases.
It remains unclear whether urinary diversion procedures improve the overall patient survival rate. Many studies are relatively old, from small cohorts, and outdated.
This study aims to determine the overall survival rates of cervical cancer patients undergoing PCN for malignant ureteral obstruction, as well as to analyze clinical variables associated with survival and to describe complications related to the procedure.
This is a retrospective, cross-sectional and observational study. Data were obtained from medical records of patients with cervical cancer undergoing PCN due to malignant obstructive uropathy between January 2019 and December 2020 at Hospital Barão de Lucena in Recife, Pernambuco (PE), Brazil.
We included patients with invasive cervical uterine malignancy (at least stages IIIB) with unilateral or bilateral hydronephrosis and renal dysfunction (AKIN stage ≥2) submitted to PCN at the time of diagnosis of neoplasia, disease progression or recurrence after previous definitive treatment.
Patients without anatomopathological biopsy results, ureteral obstruction caused by other diseases and loss of follow-up were excluded from this study.
The main objective was to estimate overall survival of these patients, defined as the date between the procedure and death. Secondary objectives were: (1) to evaluate the morbidity and complications of PCN and (2) to identify variables associated with survival.
The Centro Integrado de Saúde Amaury de Medeiros (CISAM/UPE) ethics and research committee approved the project under CAAE number 50399421.0.0000.5191, per Brazilian National Health Council Resolutions 466/12 and 510/16.
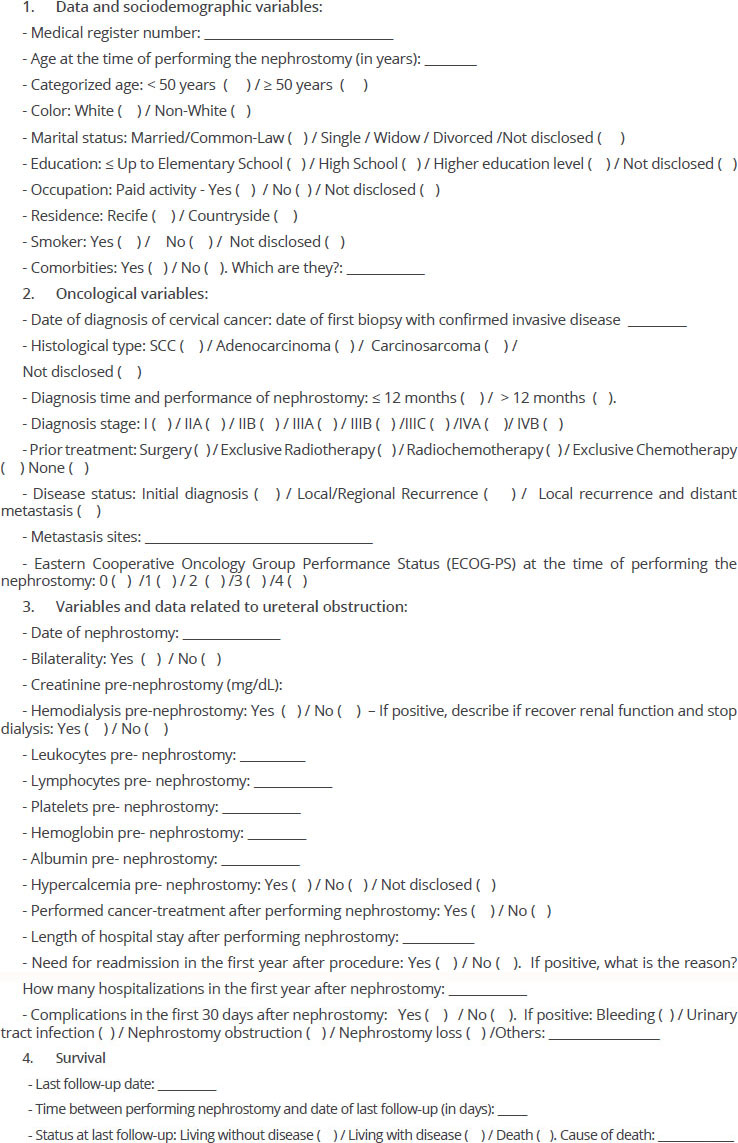
Sociodemographic, clinical-laboratory, oncological, and survival-related variables were determined. A data collection form (Appendix 1) was used to gather data from the medical records of each selected patient, and an Excel spreadsheet was created.
Qualitative variables were expressed as absolute and relative values and quantitative variables as mean, median, standard deviation, minimum, and maximum statistics. The assumed significance level was 5%. Statistical analyses were performed using SPSS – Statistical Package for Social Sciences for Windows, version 21.0.
The Kaplan-Meier estimator was used to estimate survival probability. It was first analyzed globally with no stratification. Then, it was analyzed with stratification by the covariates determined during the study. The log-rank test was used to compare survival curves according to the categories of covariates studied.
A Cox Proportional Hazards Model was adjusted to analyze the time-to-event factors considering all variables contemporaneously. The model only included covariates that were associated with a mortality rate with a significance level lower than 0.20 in the bivariate analysis.
Thirty-one (n=31) cervical cancer patients undergoing PCN were evaluated. The median age was 50 (range; 23-77 years). Race was defined as non-white in 21 patients. Most women (67.7%) studied up to elementary school.
| Variables | N = 31 |
|---|---|
| AGE (years) | |
| Mean (SD)* | 48.9 (14.1) |
| Median (minimum – maximum) | 50 (23 - 77) |
| AGE | |
| <50 years | 15 (48.4%) |
| ≥50 years | 16 (51.6%) |
| COLOR | |
| White | 10 (32.3%) |
| Non-White | 21 (67.7%) |
| MARITAL STATUS | |
| Married/Common-Law | 13 (41.9%) |
| Marriage | 15 (48.4%) |
| Single / Widow / Divorced | 3 (9.7%) |
| Not disclosed | |
| EDUCATION | |
| Up to Elementary School | 21 (67.7%) |
| High School | 3 (9.7%) |
| Not disclosed | 7 (22.6%) |
| OCCUPATION | |
| Paid activity | 14 (45.2%) |
| No paid activity | 11 (35.5%) |
| Not disclosed | 6 (19.4%) |
| RESIDENCE | |
| Recife | 16 (51.6%) |
| Countryside | 15 (48.4%) |
| SMOKER | |
| No | 14 (45.2%) |
| Yes | 11 (35.5%) |
| Not disclosed | 6 (19.4%) |
The most frequent histological subtype was squamous cell carcinoma (80.6%). Most patients were submitted to the procedure at the time of initial diagnosis (n=17) and had a performance status ≥2 (61,3%, n=19).
| Variables | N = 31 |
|---|---|
| HISTOLOGICAL TYPE | |
| SCC | 25 (80.6%) |
| Adenocarcinoma | 2 (6.5%) |
| Carcinosarcoma | 1 (3.2%) |
| Not specified | 3 (9.7%) |
| TIME FROM DIAGNOSIS | |
| <12 months | 26 (83.9%) |
| ≥12 months | 5 (16.1%) |
| STAGING AT DIAGNOSIS | |
| II-A | 1 (3.2%) |
| II-B | 5 (16.1%) |
| III-B | 6 (19,3%) |
| III-C | 3 (9.7%) |
| IV-A | 11 (35.5%) |
| IV-B | 5 (16,1%) |
| PRIOR TREATMENT | |
| Surgery | 1 (3,2%) |
| CT+RT | 14 (45.2%) |
| Exclusive CT | 1 (3.2%) |
| Surgery+CT+RT | 1 (3.2%) |
| None | 14 (45,2%) |
| DISEASE STATUS (n=31) | |
| Initial diagnosis | 17 (54,8%) |
| Local/Regional Recurrence, | 8 (26.7%) |
| Local recurrence and distant metastasis | 6 (20.0%) |
| SITES OF METASTASIS (n=11) | |
| Lung | 3 (27.3%) |
| Liver | 4 (36.4%) |
| Central nervous system | 1 (9.0%) |
| Lung + Bone + Liver | 1 (9.0%) |
| Lung+Bone | 2 (18,3%) |
| BILATERAL PCN | 22 (71.0%) |
| HD PRE-NEPHROSTOMY | 21 (67.7%) |
| HD-FREE POST-NEPHROSTOMY (n=21) | 13 (61.9%) |
| Eastern Cooperative Oncology Group Performance Status (ECOG-PS) | |
| 0-1 | 12 (38.7%) |
| ≥2 | 19 (61.3%) |
Mean serum hemoglobin (Hb) was 7.8g/dL, mean pre-procedure creatinine was 5.2mg/dL, and mean pre-procedure albumin was 2.8g/dL. The clinical and laboratory characteristics are shown in
| Variables | N = 31 |
|---|---|
| HYPERCALCEMIA (n=22) | 6 (27.3%) |
| PRE-NEPHROSTOMY PLATELETS (/mm3) | |
| Mean (SD) | 358,032.3 (136,440) |
| Median (minimum – maximum) | 371,000 (60,000 – 645,000) |
| PLATELETS (/mm3) | |
| ≤400,000 | 19 (61.3%) |
| >400,000 | 12 (38.7%) |
| PRE-NEPHROSTOMY HEMOGLOBIN (g/dL) | |
| Mean (SD) | 7.8 (2.3) |
| Median (minimum – maximum) | 7.5 (3.9 – 13.8) |
| Creatinine PRE-NEPHROSTOMY (mg/dL) | |
| Mean (SD) | 5.2 (2.8) |
| Median (minimum – maximum) | 5.2 (1.1 – 12) |
| ALBUMIN PRE-NEPHROSTOMY (n=24) | |
| Mean (SD) | 2.8 (0.6) |
| Median (minimum – maximum) | 2.8 (1.7 – 4.2) |
| NEUTROPHIL/LYMPHOCYTE RATIO (n=30) | |
| Mean (SD) | 10.4 (7.0) |
| Median (minimum – maximum) | 7.3 (2.6 – 32.3) |
The mean length of hospital stay for the procedure was 17.9 days, with a 69% complication rate in the first 30 days. The most frequent complications were bleeding (15 events) and nephrostomy tube displacement (7 events). Twenty patients have died. Main cause of death included uremia and septic shock.
| Variables | N = 31 |
|---|---|
| DAYS IN HOSPITAL POST-NEPHROSTOMY (n=30) | |
| Mean (SD) | 17.9 (13.8) |
| Median (Minimum – Maximum) | 14.5 (1 – 62) |
| 30-DAY COMPLICATION RATE (n=31) | 20 (69.0%) |
| TYPE OF COMPLICATION (10 patients presented > 1 complication) | |
| Bleeding | 15 (48,4%) |
| Nephrostomy tube displacement | 7 (22,6%) |
| Pain | 4 (12,9%) |
| UTI | 5 (16,1%) |
| ANTINEOPLASTIC TREATMENT POST-NEPHROSTOMY | 19 (61.3%) |
| Cause of death (n=20) | |
| UTI | 1 (5.0%) |
| DVT-PE | 1 (5.0%) |
| Bronchoaspiration | 1 (5.0%) |
| Bowel obstruction | 2 (10.0%) |
| Uremic syndrome | 4 (20.0%) |
| Acute Resp. Failure | 3 (15.0%) |
| Septic shock | 4 (20.0%) |
| Liver Failure | 1 (5.0%) |
| No defined cause | 3 (15.0%) |
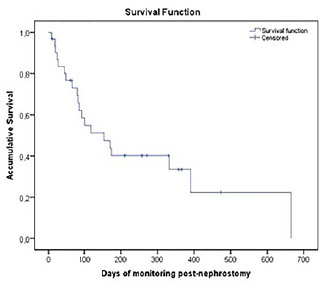
The median overall survival was 8.7 months (261 days, 95% CI: 157-365), as expressed in
Figure 1 Overall survival curve of the sample studied.
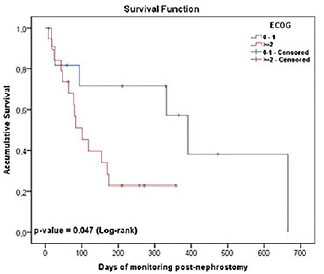
Figure 2 Survival curve per performance status.
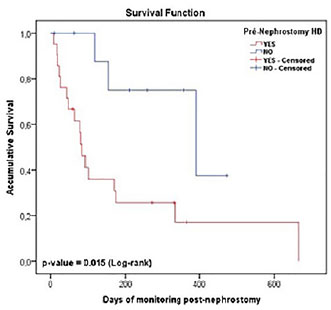
Twenty-one (21) patients required pre-nephrostomy HD, and 13 patients recovered renal function after urinary diversion. Patients who underwent HD had statistically significant worse survival (2.7 vs. 13 months, p-value of 0.01,
Figure 3 Survival curve per pre-nephrostomy HD.
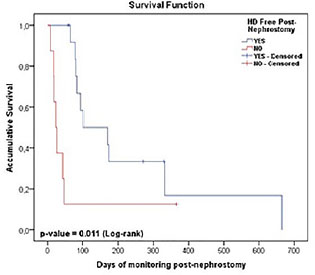
Figure 4 Survival curve per recovery of renal function post-ne-phrostomy.
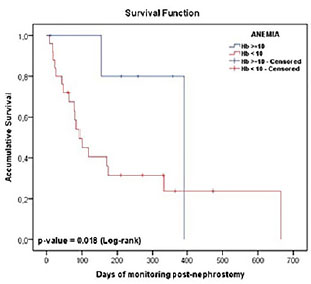
Patients with hemoglobin lower than 10g/dL had a statistically significant worse survival when comparing with patients with Hb≥10g/dL, (3.1 vs. 13 months, p-value of 0.01,
Figure 5 Survival curve per anemia.
Multivariate analysis found that patients with ECOG-PS ≥2 are approximately four times more likely to die than patients with an ECOG-PS 0-1. Patients who underwent pre-nephrostomy HD are approximately 3.7 times more likely to die than patients without pre-procedure HD, as seen in
| Variables | Multivariate | |
|---|---|---|
| RR (CI 95%) | p-value | |
| ECOG (≥2 × 0-1+) | 4.17 (1.19 – 14.52) | 0.025 |
| Pre-nephrostomy HD (Yes × No+) | 3.70 (1.11 – 12.30) | 0.033 |
| Anemia (Yes × No+) | Ns | Ns |
Despite having efficient methods for prevention and early diagnosis, cervical cancer is a challenging public health problem for developing countries.
Several studies have shown that urinary diversion can improve renal function in cervical cancer patients, although the effects of the procedure on overall survival rates are unclear.
Six patients of the sample (16,1%) were on stage IVB but only 3.2% received palliative chemotherapy. This data must be correlated with progression of disease, complications of procedure and infectious disorders.
It was also found that 54,8% of the sample comprised newly diagnosed patients; 26.7% were local-regional recurrences, and 20% were local and distant recurrences. That data corroborates that the diagnosis is still made late and, most often, in the presence of a severe complication such as malignant ureteral obstruction.
Median survival in our study was 8.7 months. Comparison with other studies is difficult, as most of them were performed with a limited number of patients. Most studies found a median overall survival of 8.9 to 34 weeks.
Twenty-one patients required renal replacement therapy before PCN (67.7%), with 13 patients fully recovering renal function and free of HD (61.9%). These findings are consistent with the literature, which has shown that among those patients requiring HD, 61.7% of them recovered renal function after the obstruction was cleared.
There were complications in 69% of the patients, with bleeding and nephrostomy tube displacement being the most prevalent. This finding is similar to those of a German study with 24 patients, which identified that 13 patients experienced bleeding after PCN (54%).
The mean post-PCN hospital stay was 17.9 days, a discrepant result from that found by Tan et al. (2019)
The leading causes of death (20 patients) in our study were septic shock and uremic syndrome. Eleven deaths were related to progression of disease and four deaths due to complications of PCNs.
Variables associated with shorter survival in our study were poor performance status, hemoglobin level <10g/dL, need of HD pre nephrostomy and not recovery of renal function after PCN. For anemia, erythropoietin has not been used as therapy. These findings are consistent with the literature.
Disease status at the time of PCN, platelet and calcium levels and neutrophil/lymphocyte ratio were not associated with survival in our study, probably due to the small sample size. Some studies have used the neutrophil/lymphocyte ratio for evaluation as a prognostic tool for patients with invasive cervical cancer, based on the hypotheses of cancer-induced elevation of inflammatory cytokines promoting angiogenesis, invasion, and hematogenous dissemination.
The strength of our study is that this is the first data on this subject in patients in the northeast of Brazil, assessing the sociodemographic factors and the overall survival rate after PCN, describing the procedure’s inherent morbidity, and evaluating possible factors associated with survival.
This study also has limitations. This is a retrospective and descriptive cohort study with a small sample size without a control arm. The absence of a post-procedure quality of life assessment makes it impossible to measure functionality, autonomy, and mental health after PCN. Sample selection bias is another limitation. As the study was developed in a tertiary hospital with HD clinic, there is a tendency to have more patients on HD (67.7% of the sample).
We conclude that patients with cervical carcinoma requiring PCN have a poor outcome with a median survival of 8.7 months in this study. ECOG-PS ≥2, Hb<10g/dL), renal failure with need of HD and not recovery of renal function after PCN adversely affect survival rates. These results clearly demonstrate that referrals for the procedure must be individualized based on patient’s desire, treatment perspectives, and functionality, since there are no clear guidelines to help us to select which patients can benefit from this procedure.
DPAL Collection and assembly of data, Conception and design, Manuscript writing
CNMT Conception and design, Data analysis and interpretation, Final approval of manuscript
MBA Collection and assembly of data, Provision of study materials or patient
FANR Conception and design, Final approval of manuscript
SBF Final approval of manuscript
Data collection
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
1. World Health Organization (WHO). Global strategy to accelerate the elimination of cervical cancer as a public health problem [Internet]. WHO, 2020.
2. Estimativa 2023: incidência de câncer no Brasil [Internet]. Ministério da Saúde/INCA, 2023.
3. Bhatla, N and Berek, JS and Fredes, MC and Denny, LA and Grenman, S and Karunaratne, K. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynecol Obstetr [online]. 2019, vol. 145, p. 129-35. https://doi.org/10.1002/ijgo.12749 Ver referência
4. Quinn, MA and Benedet, JL and Odicino, F and Maisonneuve, P and Beller, U and Creasman, WT. Carcinoma of the cervix uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynecol Obstetr [Internet] [online]. 2006, vol. 95, p. S43-S103.
5. National Comprehensive Cancer Network (NCCN). NCCN Clinical practice guidelines in Oncology: cervical cancer [Internet]. NCCN, 2020.
6. Lapitan, MCM and Buckley, BS. Impact of palliative urinary diversion by percutaneous nephrostomy drainage and ureteral stenting among patients with advanced cervical cancer and obstructive uropathy: a prospective cohort. J Obstetr Gynaecol Res [online]. 2011, vol. 37, p. 1061-70. https://doi.org/10.1111/j.1447-0756.2010.01486.x Ver referência
7. Rose, PG and Ali, S and Whitney, CW and Lanciano, R and Stehman, FB. Impact of hydronephrosis on outcome of stage III-B cervical cancer patients with disease limited to the pelvis, treated with radiation and concurrent chemotherapy: a Gynecologic Oncology Group study. Gynecol Oncol [online]. 2010, vol. 117, p. 270-5. https://doi.org/10.1016/j.ygyno.2010.01.045 Ver referência
8. Pergialiotis, V and Bellos, I and Thomakos, N and Haidopoulos, D and Perrea, DN and Kontzoglou, K. Survival outcomes of patients with cervical cancer and accompanying hydronephrosis: a systematic review of the literature. Oncol Rev [Internet] [online]. 2019, vol. 13, p. 23-29.
9. Dienstmann, R and Pinto, CS and Pereira, MT and Small, IA and Ferreira, CG. Palliative percutaneous nephrostomy in recurrent cervical cancer: a retrospective analysis of 50 consecutive cases. J Pain Sympt Manage [online]. 2008, vol. 36, p. 185-90. https://doi.org/10.1016/j.jpainsymman.2007.09.010 Ver referência
10. Emmert, C and Rassler, J and Köhler, U. Survival and quality of life after percutaneous nephrostomy for malignant ureteric obstruction in patients with terminal cervical cancer. Arch Gynecologic Obstetrics [Internet] [online]. 1997, vol. 259, p. 147-51.
11. Radecka, E and Magnusson, M and Magnusson, A. Survival time and period of catheterization in patients treated with percutaneous nephrostomy for urinary obstruction due to malignancy. Acta Radiol [online]. 2006, vol. 47, p. 328-31. https://doi.org/10.1080/02841850500492092 Ver referência
12. Cohen, PA and Jhingran, A and Oaknin, A and Denny, L. Cervical cancer. Lancet [online]. 2019, vol. 393, p. 169-82. https://doi.org/10.1016/S0140-6736(18)32470-X Ver referência
13. Maguire, PJ and Sobota, A and Mulholland, D and Ryan, JM and Gleeson, N. Incidence, management, and sequelae of ureteric obstruction in women with cervical cancer. Support Care Cancer [online]. 2019, vol. 28, p. 725-30. https://doi.org/10.1007/s00520-019-04851-9 Ver referência
14. Atuhairwe, S and Busingye, RB and Sekikubo, M and Nakimuli, A and Mutyaba, T. Urologic complications among women with advanced cervical cancer at a tertiary referral hospital in Uganda. Int J Gynecol Obstetr [online]. 2011, vol. 115, p. 282-4.
15. Souza, AC and Souza, AN and Kirsztajn, R and Kirsztajn, GM. Cervical cancer: renal complications and survival after percutaneous nephrostomy. Rev Assoc Med Bras (1992) [online]. 2016, vol. 62, p. 255-61. https://doi.org/10.1590/1806-9282.62.03.255 Ver referência
16. Plesinac-Karapandzic, V and Masulovic, D and Markovic, B and Djuric-Stefanovic, A and Plesinac, S and Vucicevic, D. Percutaneous nephrostomy in the management of advanced and terminal-stage gynecologic malignancies: outcome and complications. Eur J Gynaecol Oncol [Internet] [online]. 2010, vol. 31, p. 645-50.
17. Tan, S and Tao, Z and Bian, X and Zhao, Y and Wang, N and Chen, X. Ureteral stent placement and percutaneous nephrostomy in the management of hydronephrosis secondary to cervical cancer. Eur J Obstetr Gynecol Reprod Biol [online]. 2019, vol. 241, p. 99-103. https://doi.org/10.1016/j.ejogrb.2019.08.020 Ver referência
18. Noegroho, BS and Kurniawan, AP and Wijayanti, Z and Mustafa, A. Factors affecting survival outcome after percutaneous nephrostomy as palliative urinary diversion in obstructive uropathy due to advance cervical cancer patients. Asian Pac J Cancer Prev [online]. 2021, vol. 22, p. 1211-6. https://doi.org/10.31557/APJCP.2021.22A1211 Ver referência
19. Patel, K and Foster, NR and Kumar, A and Grudem, M and Longenbach, S and Bakkum-Gamez, J. Hydronephrosis in patients with cervical cancer: an assessment of morbidity and survival. Support Care Cancer [online]. 2014, vol. 23, p. 1303-9. https://doi.org/10.1007/s00520-014-2482-y Ver referência
20. Lee, YY and Choi, CH and Kim, HJ and Kim, TJ and Lee, JW and Lee, JH. Pretreatment neutrophil: lymphocyte ratio as a prognostic factor in cervical carcinoma. Anticancer Res [Internet] [online]. 2012, vol. 32, p. 1555-61.
21. Ittiamornlert, P and Ruengkhachorn, I. Neutrophil-lymphocyte ratio as a predictor of oncologic outcomes in stage IV-B, persistent, or recurrent cervical cancer patients treated by chemotherapy. [online]. 2019, vol. 19, p. 51.
22. Nakamura, K and Nakayama, K and Tatsumi, N and Minamoto, T and Ishibashi, T and Ohnishi, K. Prognostic significance of pre-treatment neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios in non-surgically treated uterine cervical carcinoma. Mol Clin Oncol [Internet] [online]. 2018, vol. 9, p. 138-44.
Dados de acesso insuficientes para visualização no mapa.