The oncology treatment has significantly evolved in recent decades, providing greater survival and quality of life for patients. However, these therapies often lead to adverse events that can significantly impact the oral health of individuals undergoing these approaches.
Oral mucositis is an inflammation of the oral mucosa and oral cavity, primarily caused by the toxicity of antineoplastic treatments such as chemotherapy and radiotherapy.
Patients undergoing chemotherapy who develop significant oral mucositis require supportive care measures, suchastheuseofenteralandtotalparenteral nutrition, fluid replacement, and infection prophylaxis.
Oral mucositis induced by radiotherapy also has a significant economic impact due to the costs associated with pain management, liquid diet supplements, gastrostomy tube placement, total parenteral nutrition, treatment of secondary infections, and hospitalizations.
Given this scenario, the search for effective preventive and therapeutic strategies in the prevention and management of mucositis has become a priority for the multidisciplinary team involved in oncology care.
This is a methodological study involving the review of the main scientific evidence published up to July 2023, with the objective of structuring a program for the prevention and treatment of mucositis in oncology patients. The review encompassed studies and scientific articles indexed in recognized databases such as PubMed, Scopus, and Embase, using relevant search terms such as “oral mucositis,” “prevention,” “treatment,” “oncology patients,” and their variations. Additionally, guidelines proposed by the American Society of Clinical Oncology (ASCO), the European Society of Medical Oncology (ESMO), the National Comprehensive Cancer Center (NCCN), and the Multinational Association of Supportive Care in Cancer (MASCC) were reviewed.
From this review, the best evidence regarding preventive and therapeutic approaches for oral mucositis in oncology patients was identified. Inclusion criteria considered studies involving adult patients undergoing antineoplastic treatments, such as chemotherapy, immunotherapy, and/or radiotherapy, with a focus on the occurrence, prevention, and treatment of oral mucositis. Using the PICO method (an acronym for P: population/patients; I: intervention; C: comparison/control; O: outcome), the following elements were considered for the analysis of results:
Population (P): The population of interest was composed of adult oncology patients of both sexes undergoing antineoplastic treatments. Patients with a confirmed diagnosis of malignant neoplasms based on histopathological examinations and actively undergoing treatment at the institution were included.
Intervention (I): The program’s intervention consisted of an integrated approach to preventive and therapeutic measures for oral mucositis. This included early identification of mucositis, pain and inflammation management, maintenance of proper oral hygiene, prescription of topical and systemic medications, and the implementation of specific care protocols.
Comparison (C): Since the program’s goal was to evaluate the effectiveness of preventive and therapeutic measures, a formal comparison group was not included.
Outcomes (O): Clinical outcomes assessed in the program included the incidence and severity of oral mucositis, associated complications such as secondary infections and feeding difficulties, as well as the health-related quality of life concerning oral health in patients.
Based on the PICO framework, patients undergoing chemotherapy, immunotherapy, radiotherapy in the head and neck region, and hematopoietic stem cell transplantation (HSCT) emerge as particularly vulnerable groups. These patients face an intersection of risk factors, including mucosal damage, immunosuppression, and local inflammation, making them more susceptible to mucositis. The dose, treatment duration, nutritional status (body mass index greater than 25), and the presence of comorbidities, such as diabetes or autoimmune diseases, also influence the risk. Furthermore, radiotherapy in the head and neck region and concurrent chemotherapy further increase this risk. The resulting dysfunction of salivary glands leads to dehydration, microbial colonization, trauma, and irritation of the oral mucosa. Trauma caused by prosthetics and dentition can also be considered risk factors for oral mucositis. The use of medications that sensitize the oral mucosa, such as certain antibiotics, plays a significant role in this context.
The core of the intervention lies in the identification and follow-up of patients at risk of developing mucositis, which is the responsibility of the stomatology team. This team is tasked with assessing the oral health of patients, providing preventive measures, and adopting appropriate management strategies to minimize the effects of mucositis. Additionally, patients are educated on self-care, and guidance is provided to reduce associated risks.
Regular clinical assessment: Patients undergoing antineoplastic treatment, especially those at high risk, should undergo regular clinical assessments by the stomatology team. This enables the prevention and early detection of any oral health changes that may indicate the onset of mucositis.
Monitoring risk factors: Key risk factors, such as treatment type, dosage, irradiation area, nutritional status, and comorbidities, should be closely monitored by the stomatology team.
Education and guidance: At-risk patients should receive detailed education about mucositis, its symptoms, and the importance of reporting any changes to the healthcare team. This contributes to prevention, early detection, and effective management.
Personalized preventive measures: Based on individual risk factors and initial assessments, the stomatology team can create personalized preventive strategies, including guidance on oral hygiene, the use of mucoprotective agents (e.g., vitamin E and mineral oil), and appropriate nutritional support.
Proper management: If mucositis develops, the stomatology team can implement suitable management approaches, such as laser therapy, analgesics, mouthwashes, and keratinocyte growth factors, depending on the condition’s severity.
Interdisciplinary communication: A collaborative approach with the oncology and multidisciplinary team is essential to ensure that mucositis management strategies align with the overall antineoplastic treatment.
The outcomes encompass early detection of mucositis, prevention whenever possible, and effective management when it occurs. To achieve this, the use of validated assessment tools is recommended to monitor the severity and progression of mucositis. Regular clinical examinations, conducted by trained professionals, are essential to identify the condition’s early signs. Open communication with patients is crucial for them to report symptoms such as pain, feeding difficulties, and changes in oral health.
Effective mucositis management requires an individualized multidisciplinary approach based on ASCO, ESMO, NCCN, and MASCC guidelines. The first step involves regular assessment of oral mucositis using a validated scale (e.g., Common Terminology Criteria for Adverse Events - CTCAE), covering signs and symptoms, along with regular dental examinations to identify possible infection sites and areas at risk of mucositis progression. Preventive strategies play a crucial role, including guidance on strict oral hygiene, the use of mucoprotective agents, and maintaining proper nutrition. It is also important to reduce modifiable risk factors and evaluate the need for laser therapy. Oral rinses are often used as supportive measures.
For more severe cases, pharmacological therapies may be considered. However, oral antimicrobials should not be used for prevention but can be effective in reducing microbial colonization. Additionally, prophylactic antiviral and antifungal therapy can help prevent infections. Topical anesthetics can provide pain relief but require careful administration. Gradual management begins with gentle rinses, progressing to the use of topical anesthetics and, when necessary, systemic analgesics. Treatment should be adapted to the severity of mucositis, with regular assessments to monitor effectiveness and adjust the care plan as needed. Patient education and team communication are vital throughout the process.
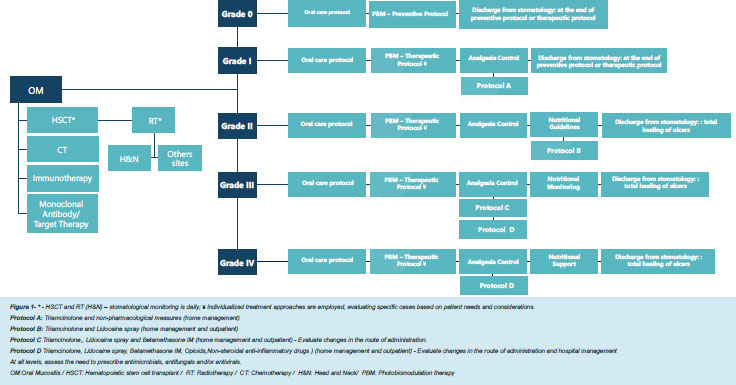
Figura 1 Flowchart of the Oncoclínicas program for preventive and therapeutic evaluation of oral mucositis.
Based on the described results, the program for the assessment and management of mucositis in oncology patients should aim to identify, prevent, and effectively manage mucositis, especially in patients undergoing chemotherapy, radiotherapy in the head and neck region, and HSCT.
Initial risk screening: All patients starting chemotherapy, early treatment with bisphosphonates, denosumab, romosozumab, everolimus, capecitabine, sunitinib, lomustine, and procarbazine, and those inserted into any care line, are evaluated by the stomatology team. This assessment will include the main complaint, evaluation of oral and extra-oral cavity, dental assessment, adverse reaction survey, pain presence, treatment type, dosage, duration, irradiation area, nutritional status, comorbidities, and the use of medications that increase oral mucosa sensitivity.
Continuous evaluation and monitoring: Patients identified as high-risk will be referred to the stomatology team for continuous evaluation and monitoring. This evaluation will include regular clinical examinations to prevent and early detect signs of mucositis, such as oral mucosa lesions, pain, and feeding difficulties.
Personalized education: Patients will receive detailed education about mucositis, its symptoms, and the importance of communicating any changes to the healthcare team. Information on proper oral hygiene, mucoprotective agents, and self-care practices will be provided in a personalized manner.
Personalized prevention plan: Based on individual risk factors, the stomatology team will develop personalized prevention plans for each patient. This will include specific measures to reduce the incidence and severity of mucositis, such as guidance on oral hygiene, the use of topical agents, laser therapy, and appropriate nutritional support.
Gradual mucositis management: If mucositis develops, the stomatology team will implement a graduated management plan, with approaches varying according to the severity of the condition. This may involve the use of analgesics, specific mouth rinses, and supportive therapies.
Interdisciplinary communication and coordination: Regular and efficient communication will be maintained between the stomatology team and the oncology team, ensuring the coordination of treatments and the alignment of mucositis prevention and management strategies with the overall antineoplastic treatment plan.
This methodological research for the proposal of an evaluation and management program for mucositis in oncology patients presented a comprehensive approach to prevent, identify, and manage this debilitating complication. The results of the analysis, based on the PICO method and the guidelines of ASCO, ESMO, NCCN, and MASCC, provided valuable insights for the creation of a program that meets the specific needs of these patients. For the structuring of this program, it was found necessary to focus on patients undergoing chemotherapy, immunotherapy, radiotherapy in the head and neck region, and HSCT as populations particularly vulnerable to mucositis. These patients share risk factors that make them susceptible to oral mucosal damage, immunosuppression, and local inflammation. The relevance of these findings lies in the possibility of directing preventive and therapeutic interventions to the highest-risk groups, maximizing the effectiveness of the implemented approaches. Furthermore, the dosage and duration of antineoplastic treatment emerged as crucial factors in susceptibility to mucositis.
Patients receiving radiotherapy in the head and neck region had an increased risk, especially of oral mucositis. Additionally, nutritional status and the presence of comorbidities, such as diabetes and autoimmune diseases, increased the likelihood of developing mucositis. Patients with a history of oral mucositis in previous chemotherapy cycles are at higher risk of developing mucositis in future cycles. Considering these factors is essential for proper and personalized care.
The program developed based on the results represents an advancement in the approach to mucositis in oncology patients. Initial risk screening, continuous evaluation, personalized education, and preventive measures are key components aimed at identifying and mitigating the development of mucositis. The flexibility of the program, which takes into account the variation in the severity of the condition, demonstrates adaptability to the individual needs of patients. A fundamental aspect of the program is interdisciplinary communication and coordination between the stomatology team, the multidisciplinary team, and the oncology team. This collaboration ensures that mucositis management strategies are aligned with the overall treatment plan, minimizing undesirable drug interactions and optimizing clinical outcomes. The interdisciplinary approach reflects the need for holistic and comprehensive care.
Despite the advances, this study has some limitations. The heterogeneity of the studied populations, treatment modalities, and the lack of specific analyses for different types of cancer can influence the generalizability of the results. Furthermore, the practical implementation of the program requires adequate resources and training for the healthcare team. Future studies should validate this program in different clinical settings, and the evaluation of long-term outcomes would be of interest. Additionally, adapting the program to address the needs of pediatric and elderly patients could further enrich the understanding of mucositis in these groups.
This study provided an in-depth view of patients at risk of developing mucositis and outlined a program aimed at improving the identification, prevention, and management of this complication. Personalization of approaches, interdisciplinarity, and care coordination emerge as fundamental pillars in optimizing the quality of life of patients during antineoplastic treatment. This study contributes to the growing understanding of mucositis and offers a practical program that can be implemented to promote better clinical outcomes and enhance the experience of oncology patients.
RLF Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing.
RMP Collection and assembly of data, Final approval of manuscript, Manuscript writing.
TBF Collection and assembly of data, Final approval of manuscript, Manuscript writing.
LFMA Collection and assembly of data, Final approval of manuscript, Manuscript writing.
ACATF Collection and assembly of data, Final approval of manuscript, Manuscript writing.
LDS Collection and assembly of data, Final approval of manuscript, Manuscript writing.
AMDC Collection and assembly of data, Final approval of manuscript, Manuscript writing.
BSA Collection and assembly of data, Final approval of manuscript, Manuscript writing.
CFL Collection and assembly of data, Final approval of manuscript, Manuscript writing.
DFA Collection and assembly of data, Final approval of manuscript, Manuscript writing.
LFA Collection and assembly of data, Final approval of manuscript, Manuscript writing.
RSS Collection and assembly of data, Final approval of manuscript, Manuscript writing.
FSDS Final approval of manuscript, Manuscript writing.
SAG Collection and assembly of data, Final approval of manuscript, Manuscript writing.
BLF Final approval of manuscript, Manuscript writing.
CGMF Final approval of manuscript, Manuscript writing.
MTL Final approval of manuscript, Manuscript writing.
PRMDM Final approval of manuscript, Manuscript writing.
CDB Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Brown, TJ and Gupta, A. Management of cancer therapy: associated oral mucositis. JCO Oncol Pract [online]. 2020, vol. 16, p. 103-9.
2. The burdens of cancer therapy. Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer [online]. 2003, vol. 98, p. 1531-9.
3. Al-Dasooqi, N and Sonis, ST and Bowen, JM and Bateman, E and Blijlevens, N and Gibson, RJ. Emerging evidence on the pathobiology of mucositis. Support Care Cancer [online]. 2013, vol. 21, p. 3233-41.
4. Pulito, C and Cristaudo, A and LaPorta, C and Zapperi, S and Blandino, G and Morrone, A. Oral mucositis: the hidden side of cancer therapy. J Exp Clin Cancer Res [online]. 2020, vol. 39, p. 210.
5. Peterson, DE and Boers-Doets, CB and Bensadoun, RJ and Herrstedt, J. ESMO Guidelines Committee. Management of oral and gastrointestinal mucosal injury: ESMO Clinical Practice Guidelines for diagnosis, treatment, and follow-up. Ann Oncol [online]. 2015, vol. 26, p. S139-S51.
6. Bensinger, W and Schubert, M and Ang, KK and Brizel, D and Brown, E and Eilers, JG. NCCN Task Force Report. prevention and management of mucositis in cancer care. J Natl Compr Canc Netw [online]. 2008, vol. 6, p. S1-21.
7. Sonis, ST and Oster, G and Fuchs, H and Bellm, L and Bradford, WZ and Edelsberg, J. Oral mucositis and the clinical and economic outcomes of hematopoietic stem-cell transplantation. J Clin Oncol [online]. 2001, vol. 19, p. 2201-5.
8. Elting, LS and Cooksley, CD and Chambers, MS and Garden, AS. Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int J Radiat Oncol Biol Phys [online]. 2007, vol. 68, p. 1110-20.
9. Campos, TM and Silva, CAPT and Sobral, APT and Sobral, SS and Rodrigues, MFSD and Bussadori, SK. Photobiomodulation in oral mucositis in patients with head and neck cancer: a systematic review and meta-analysis followed by a cost-effectiveness analysis. Support Care Cancer [online]. 2020, vol. 28, p. 5649-59.
10. Taylor, JK and Mady, LJ and Baddour, K and Iheagwara, UK and Zhai, S and Ohr, JP. A phase Ⅱ prospective trial of photobiomodulation therapy in limiting oral mucositis in the treatment of locally advanced head and neck cancer patients. World J Otorhinolaryngol Head Neck Surg [online]. 2022, vol. 8, p. 345-54.
11. Robijns, J and Nair, RG and Lodewijckx, J and Arany, P and Barasch, A and Bjordal, JM. Photobiomodulation therapy in management of cancer therapy-induced side effects: WALT position paper 2022. Front Oncol [online]. 2022, vol. 12, p. 927685.
12. Lalla, RV and Bowen, J and Barasch, A and Elting, L and Epstein, J and Keefe, DM. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer [online]. 2014, vol. 120, p. 1453-61.
13. Nekhlyudov, L and Lacchetti, C and Davis, NB and Garvey, TQ and Goldsterin, DP and Nunnink, JC. Head and Neck Cancer Survivorship Care Guideline: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Cancer Society Guideline. J Clin Oncol [online]. 2017, vol. 35, p. 1606-21.
14. Stone, PW. Popping the (PICO) question in research and evidence-based practice. Appl Nurs Res [online]. 2002, vol. 15, p. 197-8.
Dados de acesso insuficientes para visualização no mapa.