Perivascular epithelioid cell tumors, or PEComas, represent a family of mesenchymal tumors characterized by the simultaneous expression of melanocytic and muscular markers.
These tumors can arise in various anatomical sites, including the kidney, lung, bladder, prostate, pancreas, liver, falciform ligament/round ligament of the liver, breast, skin, eyes, skull base, colon, soft tissues, retroperitoneum, and the female genital tract.
Gynecological PEComas are rare, constituting approximately 25 to 30% of cases of this tumor type, with the uterine body accounting for the majority of cases (close to 72% in the retrospective study by Liu et al. (2019).
This study aims to report a case of malignant PEComa of the uterine cervix, focusing on the rarity of this tumor type, the proposed surgical treatment, the pathologist’s importance in the differential diagnosis of this neoplasm, and the follow up of this patient.
A 34-year-old female patient was referred by a gynecologist to a surgical oncology service due to vaginal bleeding and an expansive mass in the uterine cervix evolving over 5 months.
The patient had 2 previous gestations. She was using oral contraceptives and had a history of discontinuing them due to vaginal bleeding. A colpocitology had been previously conducted (1 month prior to the consultation with surgical oncology team), revealing cervical intraepithelial neoplasia (CIN) II/III. Upon speculum examination, a large friable, bleeding, exophytic mass with necrotic areas in the uterine cervix was observed, occupying the entire lateral aspect of the vaginal canal, rendering the cervical orifice unidentifiable.
Biopsy samples were collected from the mass, and the histopathological report indicated a poorly differentiated carcinoma, featuring clear and signetring-like cells, requiring immunohistochemistry (IHC) to confirm the lesion’s origin.
IHC was positive for estrogen receptor (EP1), desmin (D33) in rare cells, focal alpha-smooth muscle actin (1A4), weak and focal melan-A (A 103), HMB45, TFE3 (EP285 clone), weak p63 (DAK-p63 clone) in rare cells, vimentin (V9), and Ki-67 (MIB-1) in approximately 20% of cells, consisting with PEComa.
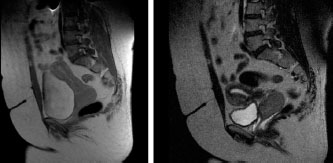
Pelvic magnetic resonance imaging (MRI) revealed a solid ovoid lesion measuring 5 cm in diameter, involving the uterine cervix and extending approximately 3 cm into the vaginal canal and no signs of parametria, rectum or bladder infiltration. (
Figure 1. Sagittal MRI section of the pelvis showing an expansive lesion in the uterine cervix, ovoid, in continuity with the vaginal vault, without evidence of involvement of the parametrium and regional lymph nodes.
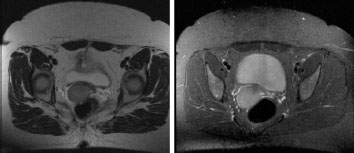
Figure 2. Axial MRI section of the pelvis showing an expansive lesion in the cervix, with a cleavage plane with the bladder and rectum.
The patient was submitted to surgical treatment. The initial idea was preserve both ovaries due to patient age and histology, but in the transoperative it was observed that the right ovary had an increase in volume and a suspicious appearance for neoplastic infiltration, despite the normal appearance at MRI. We performed a total hysterectomy with unilateral salpingo-oophorectomy and bilateral pelvic lymphadenectomy (
Figure 3. Product of total hysterectomy with unilateral salpin- go-oophorectomy and bilateral pelvic lymphadenectomy.
Postoperatively, the patient showed good progress and was referred for consultations with clinical oncology and radiation oncology to discuss adjuvant therapy options. It was decided not to proceed with any form of adjuvant therapy for this patient, who continues under clinical follow up, showing no evidence of disease after 28 months.
Gynecological PEComas are rare, with the majority being sporadic tumors, and a smaller percentage associated with complex tuberous sclerosis (CTS). PEComas of the uterine cervix are even rarer - only 16 cases have been reported in the literature until now.
| Cases | Age | History of CTS/gene mutation | Tumor size | Folpe’s criteria for agressive behavior | Treatment | Follow up |
|---|---|---|---|---|---|---|
| Case 1 | 41 | Yes | 2.2 cm | None | Total histerectomy with bilateral salpingo- oophorectomy | 35 months, without evidence of recurrence |
| Fadare et al., (2004) | Intraabdominal PEComatosis | |||||
| Case 2 | 48 | No | 2 cm | High nuclear grade | Local excision and adjuvante radiotherapy | 21 months, without. evidence of recurrence |
| Folpe et al., (2005) | ||||||
| Case 3 | 28 | No | 3 cm | None | Histerectomy and lymphadenectomy | 36 months, without evidence of recurrence |
| Folpe et al., (2005) | ||||||
| Case 4 | 25 | No | Cervical anterior lip ulceration | Infiltrative margins | Total histerectomy with bilateral salpingo- oophorectomy and lymphadenectomy | NI (no information) |
| Azad et al., (2006) | ||||||
| Case 5 | 24 | No | Cervical membranous tissue | Infiltrative margins | Local excision | 2 early cervical recurrences - 4 months after the first procedure, and 7 months after the second procedure |
| Yamamoto et al., (2010) | ||||||
|
|
|
|
|
|
| 12 months after the thirdprocedure: without evidence of recurrence |
| Case 6 | 46 | No | 3-4 cm | None | Total histerectomy with bilateral salpingo- oophorectomy + radiotherapy (external beam radiation therapy - EBRT) + immunotherapy | 36 months, without evidence of recurrence |
| Bradshaw et al., (2010) | ||||||
| Case 7 | 61 | No | 9 cm | Size > 5 cm | mTOR inhibitors | Death (8 months) |
| Wagner et al., (2010) | Pulmonary metastasis at diagnosis | |||||
| Case 8 | 59 | Yes | Non-specified | NI | Total histerectomy with bilateral salpingo- oophorectomy | NI |
| Lim et al., (2011) | ||||||
| Case 9 | 52 | No | 12 cm | Vascular invasion, necrosis, high nuclear grade | Pelvic exenteration with uterus, vagina, bladder and anal canal resection + adjuvante radiotherapy (28 fractions) | 12 months, without evidence of recurrence |
| Natella et al., (2013) | ||||||
| Case 10 | 57 | NI | 3.3 cm | Multiple bizarre giant cells, necrosis, mitotic index 2MF/5QHPF | Total histerectomy with bilateralsalpingo-oophorectomy | NI |
| Zhang et al., (2013) | ||||||
| Case 11 | 41 | Yes | 4 cm Intraabdominal PEComatosis | Infiltrative margins | Total histerectomy with bilateralsalpingo-oophorectomy | 36 months, without evidence of recurrence |
| Çelik et al., (2014) | ||||||
| Case 12 | 34 | No | 9 cm | Size > 5 cm, necrosis, infiltrative margins | Mass resection | Local recurrence after 2 months |
| Liu et al.,(2014) | | Metastatic pelvic lymph nodes after 5months | ||||
| Case 13 | 51 | No | 2.8 cm | None | Total histerectomy with bilateralsalpingo-oophorectomy | SI |
| Tajima and Koda, (2015) | ||||||
| Case 14 | 43 | No | 3 cm | None | Histerectomy | 36 months, without evidence of recurrence |
| Kovac et al., (2018) | | |||||
| Case 15 | 57 | No | 11 cm | Size > 5 cm, infiltrative margins, high nuclear grade, necrosis, mitotic index > 4 MF/10HPF | Total histerectomy with bilateral salpingo-oophorectomy and pelvic lymphadenectomy | 6 months, without evidence of recurrence |
| Mateva et al., (2019) | ||||||
| Case 16 | 55 | SI | 3 cm | None | Total histerectomy with bilateral salpingo-oophorectomy | 24 months, without evidence of recurrence |
| Tang et al.,(2023) | ||||||
| Case 17 | 34 | SI | 5.5 cm | Size > 5 cm | Total histerectomy with unilateralsalpingo-oophorectomy and bilateral pelvic lymphadenectomy | 28 months, without evidence of recurrence |
| Our case |
NI = No information; CTS = Complex tuberous sclerosis.
The first cervical PEComa was described by Fadare et al., in 2004,
While most PEComas are benign, a subgroup demonstrates aggressive behavior.
In 2005, Folpe et al.
| Category | Folpe’s criteria (2005) | Schoolmeester’s criteria (2014) | Folpe’s modified criteria -Conlon et al. (2015) |
|---|---|---|---|
| Benign | None of below criteria: • Size equal or higher 5 cm • Infiltrative growth pattern • High nuclear and cellularity grade • Mitotic index > 1M/50HPF • Necrosis • Vascular invasion | Less than four below criteria: • Size equal or higher 5 cm • High nuclear grade • Mitotic index > 1M/50HPF • Necrosis • Vascular invasion | None or one below criteria: • Infiltrative margins • Size between 5 and 10 cm • Mitotic index 2-3M/50HPF • Lymphatic and vascular invasion |
| Uncertain malignant potential | One of below criteria: • Nuclear pleomorphism/giant multinucleated cells • Size equal or higher 5 cm | One of below criteria: • Isolated important atypia • Size > 10 cm • Mitotic index equal or higher than 4M/50HPF | |
| Malignant | Two or more below criteria: • Size equal or higher 5 cm • Infiltrative growth pattern • High nuclear and cellularity grade • Mitotic index > 1M/50HPF • Necrosis • Vascular invasion | Four or more below criteria: • Size equal or higher 5 cm • High nuclear grade • Mitotic index > 1M/50HPF • Necrosis • Vascular invasion | Any grade of necrosis or two or more above criteria |
Adapted from Mateva et al., (2019)
There is a correlation between the development of PEComas and tuberous sclerosis complex, a rare genetic disease that can lead to the formation of multiple tumors (mostly benign) in various parts of the body, including the brain, skin, kidneys, heart, eyes, and lungs. In tuberous sclerosis, a mutation occurs in the TSC1 and TSC2 genes, located on chromosomes 9 and 16, respectively. In PEComas, mutations in the TSC gene can also be found, with 27% in TSC1 and 73% in TSC2, both in cases related to tuberous sclerosis complex and sporadic cases.
Another potential genetic alteration that may lead to the development of PEComas is the fusion/translocation of the TFE3 gene. These tumors typically affect younger patients without an association with tuberous sclerosis complex, displaying predominantly alveolar architecture and epithelioid cytology, low-grade nuclear atypia, rare mitoses, and minimal immunoreactivity to muscle markers.
Histologically, PEComas exhibit clear or granular cytoplasm and typically organize in a perivascular pattern, concurrently expressing myogenic markers such as smooth muscle actin (SMA) and melanocytic markers (HMB-45 and Melan-A). They present as circumscribed masses with both solid and cystic components, with rare involvement of adjacent structures or organs.
The clinical presentation is not specific, including symptoms such vaginal bleeding, pelvic/uterine masses, and pelvic and abdominal pain. Due to vaginal bleeding, cervical PEComa patients may also experience anemia.
PEComa constitutes a group of neoplasms with a challenging diagnosis, given their rarity and immunophenotypic and morphological overlap with other benign and malignant tumors.
There is still limited data regarding colpocytology in cervical PEComa.
Regarding imaging studies, on ultrasonography, cervical PEComa can be characterized by a heterogeneous area with well-defined margins or a hyperechoic appearance without a clear cleavage plane with the adjacent uterus and rich central vascularity.
The differential diagnosis of uterine PEComas is broad and includes mesenchymal neoplasms with epithelioid characteristics, with emphasis to smooth muscle tumors, endometrial stromal sarcomas, and malignant metastatic melanoma.
The most effective treatment is not well-established yet due to the rarity of cervical PEComa.
Regarding adjuvant therapy with chemotherapy and radiotherapy, studies have not consistently demonstrated benefits in this scenario.
Due to the rarity of these tumors, predicting their clinical behavior becomes challenging.
There are few reported cases of cervical PEComa in the literature, with the present report documenting 17 cases. Due to limited data, diagnosing these tumors poses a challenge, and given the uncertain biological behavior of this neoplasm, they should be considered of uncertain malignant potential. These tumors require long-term follow-up, notwithstanding the potential for late local recurrence and distant metastases. Surgical treatment, involving lesion resection with clear margins, remains the recommended therapeutic option for this type of tumor until more consistent evidence can support adjuvant approaches with chemotherapy, radiotherapy, and targeted therapy.
ASA Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
FVK Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
RVK Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
DRB Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
LFV Manuscript writing
STT Conception and design, Final approval of manuscript, Manuscript writing
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Mateva, S and Nikolova, M and Totev, T and Gorchev, G. Malignant cervical PEComa: a case report and review of the literature. JIMAB [online]. 2019, vol. 25, p. 2759-68. https://doi.org/10.5272/jimab.2019254.2759 Ver referência
2. Apitz, K. The swollen and tissue malformations of the kidney cortex. II Midsection The mesenchymal neoplasms. Virchows Arch [online]. 1943, vol. 311, p. 306-27.
3. Bonetti, F and Pea, M and Martignoni, G and Zamboni, G. PEC and sugar. Am J Surg Pathol [online]. 1992, vol. 16, p. 307-8. https://doi.org/10.1097/00000478-199203000-00013 Ver referência
4. Lombardi, W and Lombardi, LB and Ferreira, MA and Silva, FV and Ruas, SP and Vanni, FP. PEComa de colo uterino: um raro relato de caso. Relatos Casos Cir [online]. 2021, vol. 7, p. e3036. https://doi.org/10.30928/2527-2039e-20213036 Ver referência
5. Mah, SJ and Hoang, L and Lee, S and Finlayson, S and Carey, MS. Cervical PEComa: challenges in diagnosis and prognosis of a rare neoplasm. Gynecol Oncol Rep [online]. 2023, vol. 48, p. 101238. https://doi.org/10.1016/j.gore.2023.101238 Ver referência
6. Bradshaw, MJ and Folpe, AL and Croghan, GA. Perivascular epithelioid cell neoplasm of the uterine cervix: an unusual tumor in an unusual location. Rare Tumors [online]. 2010, vol. 2, p. e56. https://doi.org/10.4081/rt.2010.e56 Ver referência
7. Liu, C and Chao, WT and Lin, SC and Lau, HY and Wu, HH and Wang, PH. Malignant perivascular epithelioid cell tumor in the female genital tract. Medicine [online]. 2019, vol. 98, p. e14072. https://doi.org/10.1097/MD.0000000000014072 Ver referência
8. Fadare, O and Parkash, V and Yilmaz, Y and Mariappan, MR and Ma, L and Hileeto, D. Perivascular epithelioid cell tumor (PEComa) of the uterine cervix associated with intraabdominal “PEComatosis”: a clinicopathological study with comparative genomic hybridization analysis. World J Surg Oncol [online]. 2004, vol. 2, p. 35. https://doi.org/10.1186/1477-7819-2-35 Ver referência
9. Folpe, AL and Mentzel, T and Lehr, HA and Fisher, C and Balzer, BL and Weiss, SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol [online]. 2005, vol. 29, p. 1558-75. https://doi.org/10.1097/01.pas.0000173232.22117.37 Ver referência
10. Azad, NS and Aziz, AB and Pervez, S and Kayani, N. Uterine perivascular epithelioid cell tumour presenting as a cervical mass. J Pak Med Assoc [online]. 2006, vol. 56, p. 83-4.
11. Yamamoto, E and Ino, K and Sakurai, M and Takigawa, S and Iwase, A and Kikkawa, F. Fertility-sparing operation for recurrence of uterine cervical perivascular epithelioid cell tumor. Rare Tumors [online]. 2010, vol. 2, p. e56. https://doi.org/10.4081/rt.2010.e26 Ver referência
12. Wagner, AJ and Malinowska-Kolodziej, I and Morgan, JA and Qin, W and Fletcher, CDM and Vena, N. Clinical activity of mTOR inhibition with sirolimus in malignant perivascular epithelioid cell tumors: targeting the pathogenic activation of mTORC1 in tumors. J Clin Oncol [online]. 2010, vol. 28, p. 835-40. https://doi.org/10.1200/JCO.2009.25.2981 Ver referência
13. Lim, GS and Oliva, E. The morphologic spectrum of uterine PEC-cell associated tumors in a patient with tuberous sclerosis. Int J Gynecol Pathol [online]. 2011, vol. 30, p. 121-8. https://doi.org/10.1097/PGP.0b013e3181fa5a99 Ver referência
14. Natella, V and Merolla, F and Giampaolino, P and Bifulco, G and Mainenti, PP and Insabato, L. A huge malignant perivascular epithelioid cell tumor (PEComa) of the uterine cervix and vagina. Pathol Res Pract [online]. 2013, vol. 210, p. 186-8. https://doi.org/10.1016/j.prp.2013.10.003 Ver referência
15. Zhang, C and Pan, F and Qiao, J and Jiang, J and Du, Y and Zhao, C. Perivascular epithelioid cell tumor of the cervix with malignant potential. Int J Gynecol Obstet [online]. 2013, vol. 123, p. 72-3. https://doi.org/10.1016/j.ijgo.2013.06.013 Ver referência
16. Çelik, H and Kefeli, M and Çetinkaya, M and Yildiz, L. Perivascular Epithelioid Cell Tumor (PEComa) of the uterine cervix in a patient with tuberous sclerosis complex: a literature review. Turk Patoloji Derg [online]. 2018, vol. 34, p. 82-6. https://doi.org/10.5146/tjpath.2014.01274 Ver referência
17. Liu, F and Zhang, R and Wang, ZY and Xia, Q and Shen, Q and Shi, S. Malignant perivascular epithelioid cell tumor (PEComa) of cervix with TFE3 gene rearrangement: a case report. Int J Clin Exp Pathol [online]. 2014, vol. 7, p. 6409-14.
18. Tajima, S and Koda, K. Perivascular epithelioid cell tumor of the uterine cervix identified on a conventional cervical smear. Diagn Cytopathol [online]. 2015, vol. 43, p. 1011-6. https://doi.org/10.1002/dc.23369 Ver referência
19. Kovac, O and Babal, P and Kajo, K and Kobzova, D and Coakova, L and Cermak, M. Perivascular Epithelioid Cell Tumor (PEComa) of the uterine cervix: a case report of a 43-yr-old woman with abnormal uterine bleeding treated with hysterectomy. Int J Gynecol Pathol [online]. 2018, vol. 37, p. 492-6. https://doi.org/10.1097/PGP.0000000000000436 Ver referência
20. Tang, X and Fenf, M and Shen, Y and Chen, Q. Perivascular epithelioid cell tumor of the uterine cervix identified on the liquid‑based cytology: a case report. Diagn Pathol [online]. 2023, vol. 18, p. 7. https://doi.org/10.1186/s13000-023-01290-3 Ver referência
21. Schoolmeester, JK and Howitt, BE and Hirsch, MS and Dal Cin, P and Quade, BJ and Nucci, MR. Perivascular epithelioid cell neoplasm (PEComa) of the gynecologic tract: clinicopathologic and immunohistochemical characterization of 16 cases. Am J Surg Pathol [online]. 2014, vol. 38, p. 176-88. https://doi.org/10.1097/PAS.0000000000000133 Ver referência
22. Conlon, N and Soslow, RA and Murali, R. Perivascular epithelioid tumours (PEComas) of the gynaecological tract. J Clin Pathol [online]. 2015, vol. 68, p. 418-26. https://doi.org/10.1136/jclinpath-2015-202945 Ver referência
23. Gu, J and Wang, W and Wang, S. A retrospective case study of 13 uterine Perivascular Epithelioid Cell Neoplasm (PEComa) patients. Onco Targets Ther [online]. 2021, vol. 14, p. 1783-90. https://doi.org/10.2147/OTT.S300523 Ver referência
24. Gaducci, A and Zannoni, GF. Perivascular epithelioid cell tumors (PEComa) of the female genital tract: A challenging question for gynaecologic oncologist and pathologist. Gynecol Oncol Rep [online]. 2020, vol. 33, p. 100603. https://doi.org/10.1016/j.gore.2020.100603 Ver referência

Dados de acesso insuficientes para visualização no mapa.