Cervical cancer (CC) is characterized by a disordered replication of the organ's lining epithelium. Depending on the origin of the compromised epithelium, CC can be categorized as: squamous cell carcinoma, the most common, and which affects the squamous epithelium; and adenocarcinoma, which affects the glandular epithelium. The etiological factor that causes neoplasia in both categories is persistent infection with oncogenic types of the human papillomavirus (HPV).
In the Northeastern region of Brazil, CC is the third cause of death, with a mortality rate of 5.58/100 thousand. Also, the mortality rate from CC in Brazil, adjusted for the world population, was 4.60 deaths per100 thousand women in 2020.
Despite being known as a highly preventable disease, CC continues to be a major public health issue, having the highest incidence and mortality rates in Brazil and worldwide, being the fourth most common type of cancer among women, with approximately 570 thousand new cases every year. Also, with 311 thousand deaths per year worldwide, it is the fourth most common cause of death from cancer in women.
According to an annual report published in September 2022 by the Brazilian National Cancer Institute (Instituto Nacional do Câncer, INCA, in Portuguese),
Regarding mortality rates, according to a survey carried out in Ceará between 2014 and 2019, 1,757 deaths from CC were reported, with the highest rates being recorded in 2017 (18.4%), 2018 (17.7%), and 2019 (18.0%).
Considering that CC is preventable, actions such as vaccination against HPV comprise primary prevention actions, along with guidance on the use of condoms. Furthermore, there is a need for screening through cytopathological examination, with a focus on early detection of precancerous lesions. Primary care must also actively search for women within the target population and with overdue exams, and intervene in case of altered results (referral to a specialized service and doctor) and health education.
The therapy available for the treatment of CC includes surgical procedures and radiotherapy/chemotherapy for more advanced cases.
Due to the recurrence rates of CC, which are minimal, what is expected from the prognosis is the option for surgical intervention, as the neoplasm is considered curable in most cases. Hysterectomy can be performed when the lesion is small and restricted to the uterus and/or vagina. However, when adjacent structures are involved, the procedure of choice is pelvic exenteration.
In 1948, Alexander Brunschwig
The most common indication for exenteration is persistent carcinoma of the cervix after radiotherapy and chemotherapy (70%), followed by advanced carcinomas of the rectosigmoid colon, around 10%, for both men and women.
The main goal of the present study was to carry out an analysis of the clinicopathological factors associated with mortality and recurrence of patients with CC who underwent pelvic exenteration after the primary treatment from 2000 to 2019 at Hospital Haroldo Juaçaba, which is part of the Ceará Cancer Institute (Instituto do Câncer do Ceará, ICC, in Portuguese).
a) To evaluate the influence of clinical factors, such as age, cancer stage, histological type and presence of comorbidities, on overall survival and recurrence results in patients undergoing pelvic exenteration for CC;
b) To investigate the association between pathological characteristics, such as tumor size, lymphatic invasion and presence of metastases, and the outcomes of mortality and recurrence in patients who underwent pelvic exenteration;
c) To identify possible risk factors for postoperative surgical complications in patients undergoing pelvic exenteration due to recurrence of CC;
d) To analyze the disease-free survival rate in patients undergoing pelvic exenteration and identify possible predictive factors for local or distant recurrence;
e) To investigate the relationship between the time elapsed from primary treatment to pelvic exenteration and survival and recurrence outcomes in patients with relapsed CC.
The present work consists of an observational, cross-sectional, retrospective study, using medical records.
The analyzed data came from CC patients who underwent pelvic exenteration after the primary treatment at the Gynecologic Oncology Service of the ICC, from January 1, 2000, to December 12, /2019.
As inclusion criteria, patients who had a histological diagnosis of malignant neoplasm of the uterine cervix and underwent surgical treatment with pelvic exenteration, with recurrence after primary treatment, were considered.
The exclusion criteria were patients without a confirmed histological diagnosis of malignant neoplasm of the cervix, those who had surgical treatment other than pelvic exenteration, who had no information or incomplete medical records, or with a diagnosis of recurrence unrelated to CC.
The variables included in the analysis were:
Age;
Associated comorbidities;
Histological type of tumor;
Clinical and pathological staging;
Type of primary treatment;
Tumor size;
Degree of differentiation;
Stromal, lymphovascular, and perineural invasion;
Surgical margins;
Lymph node involvement;
Time to relapse after primary treatment;
Type of pelvic exenteration;
Postoperative complications;
Time in hospital;
Recurrences after exenteration;
Adjuvant treatment;
Follow-up and recurrence-free time;
Patients' lifespan from the date of pelvic exenteration.
The data were obtained by just one researcher, based on information from the medical records and all complementary exams carried out during patient care at the ICC from 2000 to 2019.
Data analysis was carried out using descriptive statistics, using a database created in Microsoft Excel (Microsoft Corp., Redmond, WA, USA) software, including the variables mentioned above. The data were tabulated in an Excel spreadsheet and exported to the IBM SPSS Statistics for Windows (IBM Corp., Armonk, NY, USA) software, version 20.0, in which the analyzes were carried out adopting a 95% confidence interval (95%CI) level.
The absolute and percentage frequencies of each sociodemographic and clinicopathological variable were expressed, and Kaplan-Meier curves were created to estimate the mean and median disease-free survival and overall survival times. Survival curves were crossed with sociodemographic and clinicopathological data using the Mantel-Cox logrank test. For significant values, risk ratios were calculated. The data in question were described and compared with the relevant literature.
In the present study, ethical aspects for research involving human beings were respected, as established by resolution no. 196/96 of the Brazilian National Health Council (Conselho Nacional de Saúde, CNS, in Portuguese). It will be carried out through the standards of the Brazilian Association of Technical Standards (Associação Brasileira de Normas Técnicas, ABNT, in Portuguese).
The work was submitted and approved by the Research Ethics Committee of the ICC before its beginning, under CAAE 70798223.2.0000.5528, in accordance with CNS resolution no. 466/12. The research project was approved by the Plataforma Brasil as stated in opinion 6,332,442.
The study was carried out within bioethics, keeping harmful personal information anonymous and disclosing beneficial information, always following the patients' ethical requirements.
A total of 26 patients were selected according to the research's inclusion criteria. Of these, 65.4% were under 50-years-old. Most patients did not have major comorbidities. The average length of stay was 10.7 ± 6.1 (4–26) days and the longest axis of the average tumor was of 3.93 ± 1.15 (1–6) cm.
| n | % | |
|---|---|---|
| Age (years) | ||
| Up to 50 | 17 | 65.4 |
| > 50 | 9 | 34.6 |
| SAH | ||
| No | 21 | 80.8 |
| Yes | 5 | 19.2 |
| DM | ||
| No | 24 | 92.3 |
| Yes | 2 | 7.7 |
| HIV | ||
| No | 25 | 96.2 |
| Yes | 1 | 3.8 |
| DLP | ||
| No | 25 | 96.2 |
| Yes | 1 | 3.8 |
Abbreviations: DLP, dyslipidemia; DM, diabetes mellitus; HIV, human immunodeficiency virus; SAH, systemic arterial hypertension.
Notes: Data expressed as absolute and percentage frequencies.
During the pathological analysis of the 26 patients, 20 squamous cell carcinomas predominated. Lymphovascular invasion was present in 35% of patients. Regarding the stage of the lesion, the majority were in stage II (10 patients), of which 8 were IIb.
| n | % | |
|---|---|---|
| Lymphovascular invasion | 7 | 35.0 |
| Perineural invasion | 6 | 30.0 |
| Histological type | ||
| Squamous cell carcinoma | 20 | 76.9 |
| Adenocarcinoma | 6 | 23.1 |
| Staging | ||
| I | 8 | 32.0 |
| II | 10 | 40.0 |
| III | 7 | 28.0 |
| Degree of differentiation | ||
| Moderate | 20 | 80.0 |
| Undifferentiated | 5 | 20.0 |
| Nodal metastasis | 2 | 9.5 |
| Pretreatment | ||
| Brachytherapy | 19 | 73.1 |
| Radiotherapy | 23 | 88.5 |
| Chemotherapy | 17 | 65.4 |
| Surgery | 11 | 42.3 |
Note: Data expressed as absolute and percentage frequencies.
Before pelvic exenteration, all patients underwent some type of previous treatment, brachytherapy,
| n | % | |
|---|---|---|
| Previous surgery | ||
| No | 15 | 57.7 |
| Yes, conservative | 3 | 11.5 |
| Yes, radical | 8 | 30.8 |
| Type of exenteration | ||
| Anterior | 10 | 38.5 |
| Posterior | 3 | 11.5 |
| Total | 13 | 50 |
| Reconstruction | ||
| Bricker | 10 | 38.5 |
| Colostomies | 11 | 42.3 |
| Bricker + colostomy | 5 | 19.2 |
| Surgical margins | ||
| Free | 17 | 77.3 |
| Committed | 5 | 22.7 |
| Complications | 14 | 56.0 |
| Surgical site infection (grade IIIa) | 8 | 57 |
| Anastomotic dehiscence (grade IIIb) | 2 | 14 |
| Urinary and vesicovaginal fistulas (grade IIIb) | 3 | 21 |
| Ureteral stenosis (grade IIIa) | 1 | 7 |
| Recurrence | 10 | 38.5 |
| Pelvic | 7 | 70.0 |
| Inguinal | 1 | 10.0 |
| Visceral | 2 | 20.0 |
| Death | 10 | 38.5 |
Note: Data expressed as absolute and percentage frequencies.
Of the 26 patients who underwent exenteration, 50% underwent total pelvic exenteration, of which 8 underwent reconstruction with a wet colostomy. There were 14 patients with complications related to the surgical procedure and, using the Clavien-Dindo classification, they were divided into surgical site infection (grade IIIa), anastomotic dehiscence (grade IIIb), urinary and vesicovaginal fistulas (grade IIIb), and ureteral stenosis (grade IIIa).
Regarding recurrences, 10 of the 26 patients presented pelvic,
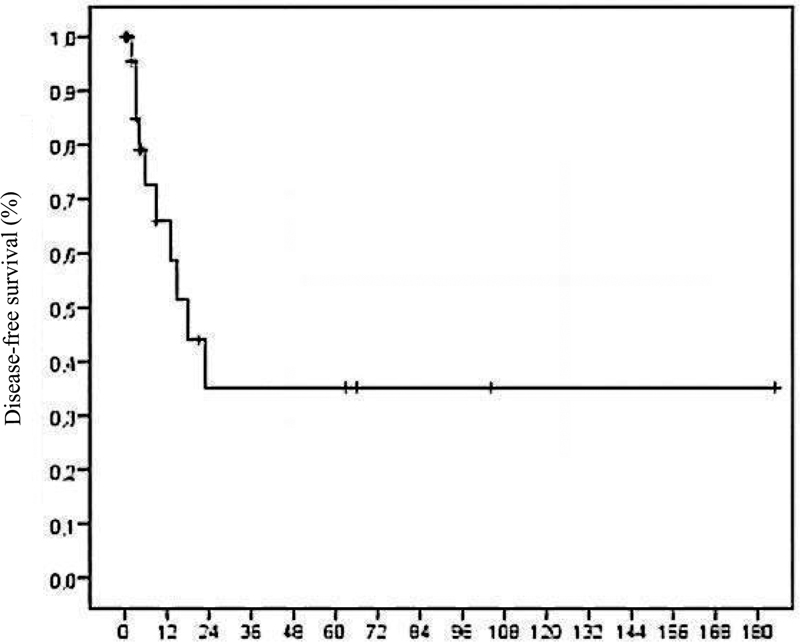
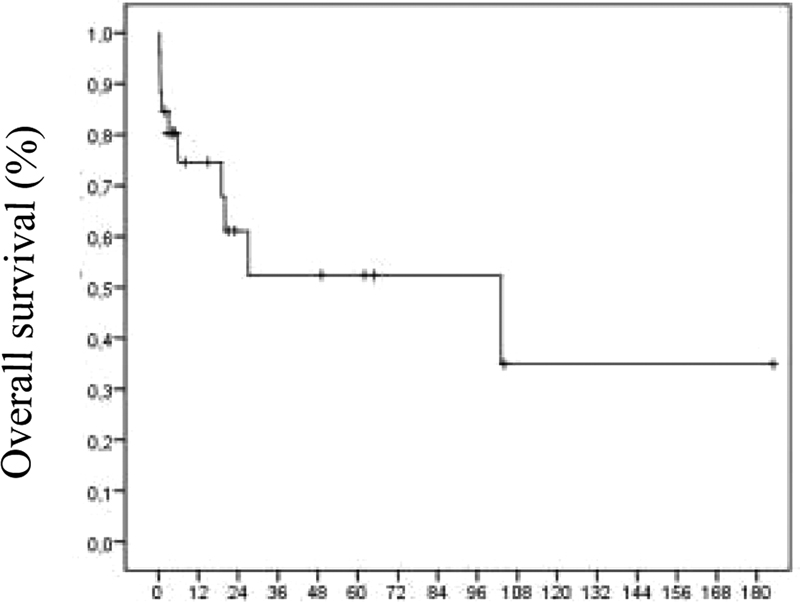
The mean disease-free time was 72 ± 22 months, with a median of 18 (95%CI = 9–27) months, and the mean overall survival was 88 ± 22 months, with a median of 103 (95%CI = 0–206) months, as shown in
Fig. 1 Time off from illness (months).
Fig. 2 Overall survival (months).
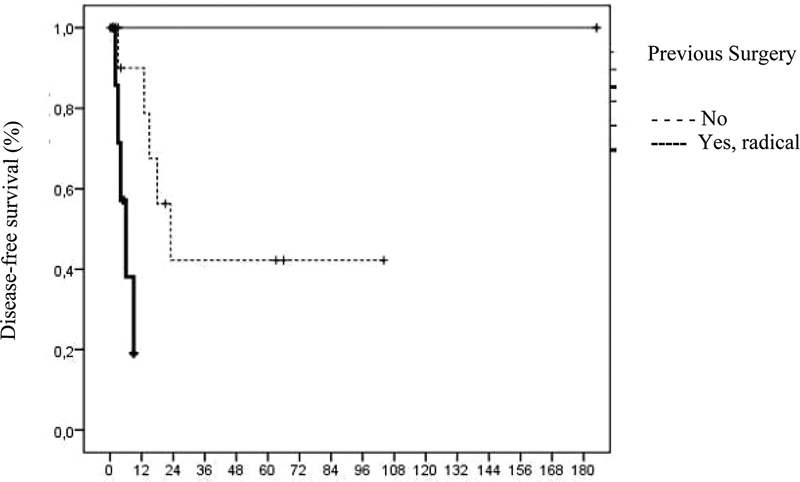
Patients with prior surgical treatment and those who underwent radical surgery had lower disease-free survival rates. In
Fig. 3 Disease-free survival of patients who have undergone prior surgical treatment (months).
| DFS | Mean ± SEM (95%CI) | Median (95%CI) | p-value | |
|---|---|---|---|---|
| Age at diagnosis (years) | ||||
| Up to 50 | 13 (76.5%) | 109.14 ± 30.24 (49.88–168.41) | – | 0.177 |
| > 50 | 3 (33.3%) | 19.14 ± 7.73 (4.00–34.29) | 15 (0–38.10) | |
| Histological type | ||||
| Squamous cell carcinoma | 13 (65.0%) | 83.88 ± 25.64 (33.63–134.13) | 23 (7.88–38.12) | 0.222 |
| Adenocarcinoma | 3 (50.0%) | 10.80 ± 2.89 (5.13–16.47) | 15 | |
| Staging | ||||
| I | 7 (87.5%) | 126.33 ± 47.90 (32.45–220.22) | – | 0.358 |
| II | 4 (40.0%) | 19.83 ± 8.37 (3.42–36.25) | 6 (0–22.63) | |
| III | 4 (57.1%) | 49.50 ± 20.66 (9.01–89.99) | 15 (10.83–19.17) | |
| Degree of differentiation | ||||
| Moderate | 11 (55.0%) | 39.46 ± 12.69 (14.60–64.33) | 18 (3.55–32.45) | 0.794 |
| Undifferentiated | 4 (80.0%) | 15.00 ± 0.00 (15.00–15.00) | 15 | |
| Brachytherapy | ||||
| No | 4 (57.1%) | 31.20 ± 12.83 (6.05–56.35) | 15 (0–34.32) | 0.972 |
| Yes | 12 (63.2%) | 65.46 ± 27.98 (10.63–120.30) | 18 (6.34–29.66) | |
| Radiotherapy | ||||
| No | 2 (66.7%) | 124.33 ± 49.53 (27.25–221.42) | – | 0.378 |
| Yes | 14 (60.9%) | 34.81 ± 12.59 (10.14–59.48) | 15 (7.40–22.60) | |
| Chemotherapy | ||||
| No | 3 (33.3%) | 24.88 ± 8.70 (7.82–41.93) | 13 (0–29.63) | 0.499 |
| Yes | 13 (76.5%) | 100.33 ± 33.19 (35.28–165.38) | – | |
| Surgery | ||||
| No | 16 (66.7%) | 81.54 ± 24.47 (33.58–129.50) | 23 (10.81–35.19) | 0.016 |
| Yes | 0 (.0%) | 4.50 ± 1.50 (1.56–7.44) | 3 | |
| Previous surgery | ||||
| No | 10 (66.7%) | 52.58 ± 15.36 (22.48–82.69) | 23 (10.90–35.10) | 0.009 |
| Yes, conservative | 3 (100.0%) | – | – | |
| Yes, radical | 3 (37.5%) | 5.86 ± 1.19 (3.52–8.19) | 6 (1.90–10.10) | |
| Lymphovascular invasion | ||||
| No | 8 (61.5%) | 26.26 ± 9.90 (6.86–45.65) | 13 (3.01–22.99) | 0.667 |
| Yes | 4 (57.1%) | 15.33 ± 5.33 (4.88–25.78) | 23 | |
| Perineural invasion | ||||
| No | 9 (64.3%) | 26.10 ± 9.30 (7.88–44.32) | 15 (10.08–19.92) | 0.002 |
| Yes | 3 (50.0%) | 2.80 ± 0.22 (2.37–3.23) | 3 (2.17–3.83) | |
| Type | ||||
| Previous | 7 (70.0%) | 124.44 ± 28.55 (68.49–180.40) | – | 0.127 |
| Posterior | 2 (66.7%) | 63.50 ± 28.64 (7.37–119.63) | 23 | |
| Total | 7 (53.8%) | 11.27 ± 2.13 (7.10–15.45) | 13 (5.37–20.63) | |
| Reconstruction | ||||
| Bricker | 7 (70.0%) | 124.44 ± 28.55 (68.49–180.40) | – | 0.490 |
| Wet colostomy | 6 (54.5%) | 28.84 ± 14.78 (0.00–57.80) | 15 (5.12–24.88) | |
| Bricker + colostomy | 3 (60.0%) | 13.50 ± 4.50 (4.68–22.32) | 9 | |
| Margins | ||||
| Free | 11 (64.7%) | 28.33 ± 8.89 (10.89–45.76) | 18 (10.69–25.31) | 0.659 |
| Committed | 3 (60.0%) | 12.33 ± 4.25 (4.00–20.67) | 13 (0–29) | |
| Nodal metastasis | ||||
| No | 12 (63.2%) | 22.94 ± 7.86 (7.53–38.35) | 15 (8.27–21.73) | 0.132 |
| Yes | 1 (50.0%) | 3.00 ± 0.71 (1.61–4.39) | 2 | |
| Complications | ||||
| No | 4 (36.4%) | 21.87 ± 8.20 (5.81–37.94) | 15 (0–30.30) | 0.185 |
| Yes | 11 (78.6%) | 83.00 ± 37.30 (9.89–156.11) | 23 (1.53–44.47) |
Abbreviations: 95%CI, 95% confidence interval; DFS, disease-free survival; SEM, standard error of the mean.
Notes: *p < 0.05, Mantel-Cox logrank test. The means, standard error, and median disease-free survival were calculated based on the construction of Kaplan-Meier curves.
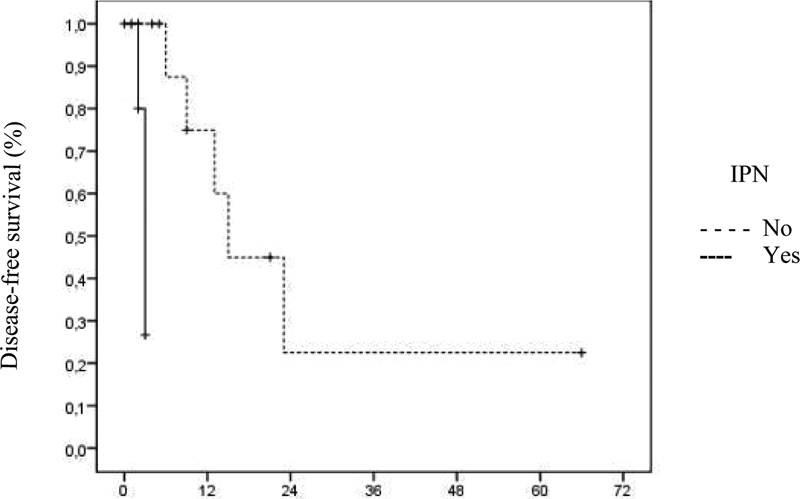
The disease-free survival of patients with perineural invasion was 430.9 (95%CI = 0.1–3,500.0) times lower than that of patients without perineural invasion, as seen in
Fig. 4 Disease-free survival of patients with perineural invasion (months).
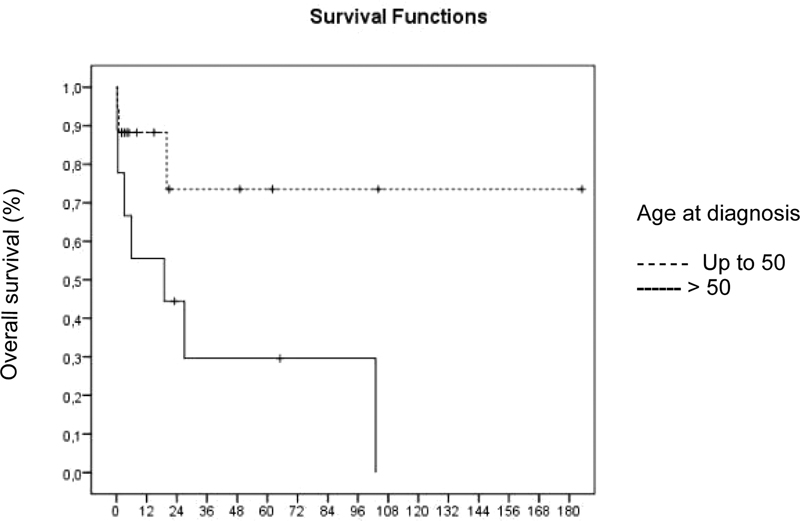
Fig. 5 Overall survival of patients aged up to 50 years.
| OS (%) | Mean ± SEM (95%CI) | Median (95%CI) | p-value | |
|---|---|---|---|---|
| Age at diagnosis (years) | ||||
| Up to 50 | 14 (82.4%) | 139.06 ± 25.31 (89.45–188.67) | – | 0.030 |
| > 50 | 2 (22.2%) | 37.73 ± 16.35 (5.68–69.78) | 19 (0–56.98) | |
| Histological type | ||||
| Squamous cell carcinomna | 13 (65.0%) | 95.61 ± 24.32 (47.94–143.28) | 103 (0–246.44) | 0.327 |
| Adenocarcinoma | 3 (50.0%) | 23.27 ± 9.41 (4.83–41.70) | 19 (0–42.95) | |
| Staging | ||||
| I | 7 (87.5%) | 161.94 ± 21.57 (119.65–204.22) | – | 0.468 |
| II | 5 (50.0%) | 51.82 ± 19.59 (13.42–90.21) | 27 (13.24–40.76) | |
| III | 4 (57.1%) | 54.62 ± 20.77 (13.91–95.32) | 19 | |
| Degree of differentiation | ||||
| Moderate | 11 (55.0%) | 57.63 ± 12.29 (33.54–81.72) | 103 (15.16–190.84) | 0.848 |
| Undifferentiated | 4 (80.0%) | 19.00 ± 0.00 (19.00–19.00) | 19 | |
| Previous brachytherapy | ||||
| No | 2 (28.6%) | 25.23 ± 9.89 (5.84–44.61) | 19 (0–52.36) | 0.086 |
| Yes | 14 (73.7%) | 110.06 ± 27.07 (57.01–163.11) | 103 (0–245.14) | |
| Previous radiotherapy | ||||
| No | 2 (66.7%) | 130.00 ± 44.91 (41.98–218.02) | – | 0.402 |
| Yes | 14 (60.9%) | 56.90 ± 12.99 (31.44–82.37) | 27 (0–92.77) | |
| Previous chemotherapy | ||||
| No | 5 (55.6%) | 64.92 ± 19.27 (27.15–102.69) | 103 | 0.748 |
| Yes | 11 (64.7%) | 106.74 ± 26.83 (54.16–159.32) | – | |
| Previous treatment with surgery | ||||
| No | 16 (66.7%) | 100.19 ± 22.97 (55.18–145.21) | 103 (0–240.56) | 0.135 |
| Yes | 0 (0.0%) | 13.00 ± 7.00 (0.00–26.72) | 6 | |
| Type of previous surgery | ||||
| No | 10 (66.7%) | 60.41 ± 15.45 (30.13–90.69) | – | 0.274 |
| Yes, conservative | 3 (100.0%) | – | – | |
| Yes, radical | 3 (37.5%) | 46.54 ± 21.03 (5.32–87.76) | 20 (0–47.89) | |
| Lymphovascular invasion | ||||
| No | 9 (69.2%) | 38.63 ± 10.35 (18.34–58.92) | – | 0.697 |
| Yes | 4 (57.1%) | 15.40 ± 3.68 (8.20–22.60) | 20 (0–45.24) | |
| Perineural invasion | ||||
| No | 10 (71.4%) | 42.55 ± 9.17 (24.57–60.53) | – | 0.241 |
| Yes | 3 (50.0%) | 13.29 ± 4.65 (4.17–22.41) | 20 | |
| Type | ||||
| Previous | 7 (70.0%) | 111.03 ± 29.96 (52.32–169.74) | 103 (0–223.04) | 0.246 |
| Posterior | 2 (66.7%) | 69.53 ± 28.14 (14.38–124.69) | – | |
| Total | 7 (53.8%) | 20.35 ± 6.41 (7.79–32.91) | 19 (0–44.20) | |
| Reconstruction | ||||
| Bricker | 7 (70.0%) | 111.03 ± 29.96 (52.32–169.74) | 103 (0–223.04) | 0.454 |
| Colostomy | 6 (54.5%) | 44.60 ± 18.05 (9.22–79.99) | 19 (0–44.72) | |
| Bricker + colostomy | 3 (60.0%) | 30.60 ± 9.08 (12.79–48.41) | 27 (0–64.79) | |
| Margins | ||||
| Free | 10 (58.8%) | 30.68 ± 8.75 (13.52–47.84) | 27 (3.04–50.96) | 0.945 |
| Committed | 3 (60.0%) | 16.60 ± 3.50 (9.74–23.46) | 20 (0–47.62) | |
| Nodal metastasis | ||||
| No | 11 (57.9%) | 26.73 ± 8.28 (10.51–42.96) | 20 (13.03–26.97) | 0.513 |
| Yes | 1 (50.0%) | 3.50 ± 0.35 (2.81–4.19) | 3 | |
| Complications | ||||
| No | 5 (45.5%) | 47.31 ± 17.26 (13.48–81.15) | 27 (17.57–36.43) | 0.547 |
| Yes | 10 (71.4%) | 132.31 ± 22.26 (88.68–175.95) | – | |
| Recurrence | ||||
| No | 12 (75.0%) | 138.90 ± 19.96 (99.77–178.03) | – | 0.340 |
| Yes | 4 (40.0%) | 46.87 ± 17.23 (13.10–80.63) | 27 (17.54–36.46) |
Abbreviations: 95%CI, 95% confidence interval; SEM, standard error of the mean. Notes: *p < 0.05, Mantel-Cox logrank test. The means, standard error, and median of disease-free survival were calculated based on the construction of Kaplan-Meier curves.
Pelvic exenteration surgery, long considered quite aggressive and technically complex, has had its morbidity and mortality reduced due to advances in surgical technique, preoperative care, better patient selection, the advent of new broad-spectrum antibiotics, and intensive care units. This procedure is reserved for cases of local recurrence or persistence of cancer in the cervix, endometrium, vulva, and vagina after radiochemotherapy treatment. Some of these patients have already undergone surgery for the primary treatment of gynecological cancer, with hysterectomy and iliac-obturator lymphadenectomy, which can make the procedure even more difficult.
In the present series of cases, the age range found in the research sample corroborates other references from the scientific community. In a survey carried out in a university hospital with 37 patients, the median age of the patients was 60-years-old, with an interquartile range of 47 to 67-years-old, which is also close to our sample.
With regard to the comorbidities that may affect patients after the exenteration to which the patient was subjected, the main ones are surgical complications, with patients' pasts listed as possible reasons for them. Diabetes, repeated preoperative chemoradiotherapy, and history of pelvic surgery were also noted.
In the study by Benn et al.,
In a cohort carried out with 138 patients in the United States, 69 patients had systemic arterial hypertension, and 24 patients had diabetes mellitus. Furthermore, 74.6% of the sample had some type of comorbidity and/or previous risk factor.
A study from 2019 found that the presence of more than three comorbidities was independently associated with severe postoperative complications after pelvic exenteration.
Regarding the histological type of the lesions, in a master's thesis defended by Barros,
The results of 7 patients with lymphovascular invasion lesions were obtained here. According to the literature, this factor directly affects the survival of affected patients as it represents a poor prognosis.
In a cohort study carried out by Zanini et al., perineural invasion was found in the entire sample, also contributing to disease-free survival.
Regarding treatment, a retrospective cohort study carried out in the state of Rio Grande do Sul demonstrated that 66.5% of the sample were treated for locally-advanced tumors with radiotherapy and chemotherapy, similar to the present study.
In an American study, five patients with pelvic nodal persistence after initial chemoradiation received radical surgery, of which four were radical hysterectomies with lymph node dissection.
Pelvic exenteration is a very extensive and long operation, associated with a high rate of perioperative morbidity and mortality.
As in the present research, a retrospective study included a sample that was mostly subjected to anterior pelvic exenteration (47 patients) compared to posterior pelvic exenteration (18 patients).
Regarding the surgical margins of the sample of the present study, 17 were free and 5 were compromised by the procedure, a result similar to that found by Chiantera et al.
Research regarding the technique of laterally extended endopelvic resection (LEER), which is widely used in the modality in question, reports that such conduct significantly contributed to obtaining free margins of lesions in the overwhelming majority of procedures performed, being effective in cases with pelvic tumors in 97%.
Free resection margins are a fundamental factor for good prognosis, while margins involving the lymphovascular region and anterior organs have a negative effect on patient survival.
The Bricker reconstruction technique is considered the gold standard for urinary reconstructions after exenteration for gynecological recurrence in patients undergoing radiotherapy. In the research by Barros et al.,
In 2012, a study was carried out to evaluate the complications associated with double-mouth wet colostomy in the first 6 months after pelvic exenteration, compared to separate urinary and fecal diversion. The wet colostomy presented the advantage of shorter operative times and reduction of important complications, such as anastomotic leaks, being able to overcome the discomfort of incontinent stomas in a heavily irradiated population that, overall, has poor long-term survival; as such, it was favorable in relation to the more technically challenging separate urinary diversions.
If complete urinary and intestinal reconstruction is impossible separately, double-barreled wet colostomy is used, which proposes the simultaneous diversion of two systems to a single stoma, eliminating the need to manipulate the small intestine, providing a reduction in the risk of develop a fistula or dehiscence, reducing surgical procedure time without increasing morbidity, in addition to being more comfortable for the patient.
These results are in balance with those found in this research, since 10 patients underwent the Bricker technique and 8 a wet colostomy. It is worth mentioning that, regardless of the chosen approach, the patients achieved reasonable standards of disease-free survival.
Regarding the survival and death of patients after pelvic exenteration in CCU, a Piauí research reported 5 cases,
In the aforementioned study, most of the patients in the sample were under 50-years-old. As we can see in
In a study by Li et al.,
Retrospective study on the survival of patients undergoing curative pelvic exenteration obtained an overall result of 40.7%. In a cumulative 5-year period of analysis, survival for the entire cohort was 38%, and the research authors consider pelvic exenteration a valid therapeutic option for patients with persistent or recurrent advanced primary CC.
Quality of life, risk of postoperative complications, and life expectancy must be balanced. When the overall median survival is low, assessment of long-term oncological outcomes is mandatory. However, an improved preoperative assessment, following validated clinical protocols, must be carried out, evaluating data such as BMI, preoperative hemoglobin, comorbidities, previous treatments, and likely surgical complexities.
Pelvic exenteration offers about a 50% chance of saving patients with cancer of the lower and middle female genital tract that persists, recurs, or arises again after pelvic radiotherapy, in cases where the tumor's diameter does not exceed 5 cm, there are no metastases, or transperitoneal dissemination and R0 resection is achieved. New surgical modifications, such as total mesovisceral excision and laterally extended endopelvic resection, may increase the rate of R0 resections, even for tumors fixed to the lateral wall of the pelvis (except in the area of the sciatic foramen), which were previously considered a contraindication to exenteration pelvic. Although treatment-related mortality has decreased considerably, to less than 5%, severe morbidity is still high (> 50%), mainly due to compromised healing, immunological deficits of the irradiated tissue, and the use of complex techniques.
In the present study, the recurrence rate after pelvic exenteration was of 38.5%, with pelvic recurrences being the most common (70%). This finding is in line with previous literature that suggests that pelvic exenteration, despite being a radical procedure, does not guarantee complete eradication of the disease, especially in cases where the cancer has advanced beyond the local stage or where there is involvement of adjacent structures.
The present study has some limitations, including its retrospective nature, which may introduce recall bias and confidence in the accuracy of medical records. Furthermore, the cross-sectional design of the study prevents us from establishing causality between clinical/pathological factors, mortality, and recurrence outcomes. The sample size of 26 patients may also limit the generalization of the results, as it may not be representative of the broader population of CC patients undergoing pelvic exenteration. Furthermore, the study was conducted at a single institution, which may not reflect the diversity of practices and outcomes in different healthcare settings. The analysis did not take into account possible confounding variables that could influence results, such as socioeconomic status, access to healthcare, and patients' adherence to follow-up treatments.
Despite these limitations, this study provides valuable information about the clinicopathological factors associated with CC outcomes after pelvic exenteration and highlights the need for further research in this area.
Pelvic exenteration is a complex surgical procedure with significant risks and is indicated for selected patients with advanced CC. The study found that certain factors, such as perineural invasion and prior surgical treatment, were associated with poorer disease-free survival rates. Additionally, older patients (> 50 years) had a lower overall survival rate compared with younger ones. Despite the high morbidity and mortality associated with pelvic exenteration, this procedure can offer long-term disease control, and even cure it in some cases. However, it is crucial to consider the potential impact on quality of life and sexual function.
These findings underscore the importance of careful patient selection and the need for continued efforts in CC prevention and early detection, particularly among younger women.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. [citado 16 fev 2023] [online]. Available from: <https://antigo.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//dados_e_numeros_colo_22marco2023.pdf>.
2. [citado 16 fev 2023] [online]. Available from: <https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//informativo21.pdf>.
3. International Agency for Research on Cancer (IARC). Cancer today. WHO, 2020.
4. [citado 16 fev 2023] [online]. Available from: <https://www.gov.br/inca/pt-br/assuntos/gestor-e-profissional-de-saude/controle-do-cancer-do-colo-do-utero/dados-e-numeros/mortalidade>.
5. . Res Soc Dev 2022;11(05): [online]. Available from: <>.
6. Holanda, J CR and Araújo, M HHPO and Nascimento, W G and Gama, M PA and Sousa, C SM. Uso do protocolo de saúde da mulher na prevenção do câncer de colo do útero. Rev Baiana Enferm [online]. 2021, vol. •••, p. 35.
7. Laporte, G A and Zanini, L AG and Zanvettor, P H. Guidelines of the Brazilian Society of Oncologic Surgery for pelvic exenteration in the treatment of cervical cancer. J Surg Oncol [online]. 2020, vol. 121, p. 718-729.
8. . Esc Anna Nery 2018;22(04): [online]. Available from: <>.
9. Filho, R CS. Indicações e complicações da exenteração pélvica no câncer ginecológico. Feminina. [online]. 2014, vol. 42, p. 77-82.
10. Petruzziello, A and Kondo, W and Hatschback, S B. Surgical results of pelvic exenteration in the treatment of gynecologic cancer. World J Surg Oncol [online]. 2014, vol. 12, p. 279.
11. Brunschwig, A. Complete excision of pelvic viscera for advanced carcinoma; a one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy. Cancer [online]. 1948, vol. 1, p. 177-183.
12. Höckel, M and Dornhöfer, N. Pelvic exenteration for gynaecological tumours: achievements and unanswered questions. Lancet Oncol [online]. 2006, vol. 7, p. 837-847.
13. Vieira, S C and Costa, D R and Meneses, A D and Borges e Silva, J and Oliveira, A KS and Sousa, R B. Exenteração pélvica para câncer do colo uterino recidivado pós-radioterapia: experiência de um centro terciário do Nordeste brasileiro. Rev Bras Ginecol Obstet [online]. 2009, vol. 31, p. 22-27.
14. Lewandowska, A and Szubert, S and Koper, K and Koper, A and Cwynar, G and Wicherek, L. Analysis of long-term outcomes in 44 patients following pelvic exenteration due to cervical cancer. World J Surg Oncol [online]. 2020, vol. 18, p. 234.
15. Matsuo, K and Mandelbaum, R S and Adams, C L and Roman, L D and Wright, J D. Performance and outcome of pelvic exenteration for gynecologic malignancies: A population-based study. Gynecol Oncol [online]. 2019, vol. 153, p. 368-375.
16. de Gregorio, N and de Gregorio, A and Ebner, F. Pelvic exenteration as ultimate ratio for gynecologic cancers: single-center analyses of 37 cases. Arch Gynecol Obstet [online]. 2019, vol. 300, p. 161-168.
17. Li, L and Ma, S Q and Tan, X J and Zhong, S and Wu, M. Pelvic Exenteration for Recurrent and Persistent Cervical Cancer. Chin Med J (Engl) [online]. 2018, vol. 131, p. 1541-1548.
18. Benn, T and Brooks, R A and Zhang, Q. Pelvic exenteration in gynecologic oncology: a single institution study over 20 years. Gynecol Oncol [online]. 2011, vol. 122, p. 14-18.
19. Tortorella, L and Casarin, J and Mara, K C. Prediction of short-term surgical complications in women undergoing pelvic exenteration for gynecological malignancies. Gynecol Oncol [online]. 2019, vol. 152, p. 151-156.
20. Barros, A V. . , .
21. Valério, M P. Câncer de colo de útero: do diagnóstico ao tratamento. Brazilian J Dev. [online]. 2022, vol. 8, p. 20235-20241.
22. . National Comprehensive Cancer Network; 2017 [citado 17 mar 2023] [online]. Available from: <http://www.nccn.org/>.
23. Yang, K and Cai, L and Yao, L. Laparoscopic total pelvic exenteration for pelvic malignancies: the technique and short-time outcome of 11 cases. World J Surg Oncol [online]. 2015, vol. 13, p. 301.
24. Castro, L M and Vieira, S C. Sobrevida após exenteração pélvica em câncer de colo do útero recidivado: uma série de cinco casos. Femina [online]. 2021, vol. 49, p. 444-448.
25. Cibula, D and Zikan, M and Fischerova, D. Pelvic floor reconstruction by modified rectus abdominis myoperitoneal (MRAM) flap after pelvic exenterations. Gynecol Oncol [online]. 2017, vol. 144, p. 558-563.
26. Lin, A J and Ma, S and Markovina, S. Clinical outcomes after isolated pelvic failure in cervical cancer patients treated with definitive radiation. Gynecol Oncol [online]. 2019, vol. 153, p. 530-534.
27. Karmaniolou, I and Arkadopoulos, N and Vassiliou, P. Pelvic Exenteration Put into Therapeutical and Palliative Perspective: It Is Worth to Try. Indian J Surg Oncol [online]. 2018, vol. 9, p. 552-557.
28. Chiantera, V and Rossi, M and De Iaco, P. Survival after curative pelvic exenteration for primary or recurrent cervical cancer: a retrospective multicentric study of 167 patients. Int J Gynecol Cancer [online]. 2014, vol. 24, p. 916-922.
29. Backes, F J and Tierney, B J and Eisenhauer, E L and Bahnson, R R and Cohn, D E and Fowler, J M. Complications after double-barreled wet colostomy compared to separate urinary and fecal diversion during pelvic exenteration: time to change back?. Gynecol Oncol [online]. 2013, vol. 128, p. 60-64.
30. Rutledge, F N and McGuffee, V B. Pelvic exenteration: prognostic significance of regional lymph node metastasis. Gynecol Oncol [online]. 1987, vol. 26, p. 374-380.
Dados de acesso insuficientes para visualização no mapa.